
Журнал «Медицина неотложных состояний» Том 19, №1, 2023
Вернуться к номеру
Особливості коагуляційного гемостазу в пацієнтів з політравмою
Авторы: Вишинська М.Б.
Львівський національний медичний університет імені Данила Галицького, м. Львів, Україна
Рубрики: Медицина неотложных состояний
Разделы: Клинические исследования
Версия для печати
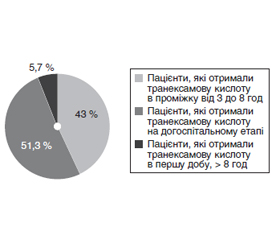
Актуальність. Посттравматична коагулопатія розвивається в 40 % пацієнтів із травмою і є найчастішою причиною смерті травмованих хворих. Мета: вивчити й проаналізувати зміни показників коагуляційного гемостазу, оцінити частоту виникнення дрібних кровотеч у пацієнтів з політравмою. Матеріали та методи. Проведено проспективне обсерваційне когортне дослідження серед пацієнтів, які перебували на лікуванні в Комунальному некомерційному підприємстві «Перше територіальне медичне об’єднання м. Львова», відокремленому підрозділі «Лікарня святого Луки» з 01.01.2021 по 01.08.2022 з діагнозом «політравма» у відділенні анестезіології з ліжками інтенсивної терапії. Включено 35 пацієнтів. Оцінювали включення в лікування транексамової кислоти в першу добу після отримання політравми, розподіляючи отримані дані за часовими інтервалами: догоспітальний етап і перші 3 години з моменту надходження на лікування; 3–8 год і 8–24 год з моменту надходження на лікування. Коагуляційний гемостаз оцінювали за показниками міжнародного нормалізованого співвідношення (INR), активованого часткового тромбопластинового часу (АЧТЧ), рівнем загального фібриногену і D-димерів. Виникнення дрібних кровотеч встановлювали візуально. Етапи дослідження: перша доба (d1), третя доба (d3) після отримання політравми. Результати. Досліджено показники коагуляційного гемостазу в пацієнтів з політравмою і виявлено, що на першу добу виникає вірогідне зростання протромбінового часу, зниження протромбінового індексу і рівня загального фібриногену, зростання INR та АЧТЧ. На третю добу з моменту отримання травми в пацієнтів групи всі досліджувані показники, за винятком АЧТЧ, вірогідно не відрізнялися від аналогічних показників контрольної групи. Рівень D-димерів на всіх етапах дослідження був вищим за показники норми. Оцінивши частоту виникнення дрібних кровотеч у пацієнтів на 1-шу — 5-ту добу після травми, виявили, що такі кровотечі не були пов’язані з порушеннями в системі коагуляційного гемостазу. Висновки. Оцінивши показники коагуляційного гемостазу, виявили, що на третю добу після травми нормалізуються всі показники, окрім АЧТЧ. Встановлено, що виникнення дрібних кровотеч не було пов’язане з порушеннями в системі коагуляційного гемостазу, тому, імовірно, вони можуть бути пов’язані із судинно-тромбоцитарними змінами або порушеннями в ланці фібринолізу.
Background. Post-traumatic coagulopathy develops in 40 % of trauma patients and is the most common cause of death in them. The objective was to study and analyze changes in indicators of coagulation hemostasis, to evaluate the frequency of minor bleedings in patients with polytrauma. Materials and methods. A prospective observational cohort study was conducted among 35 patients with a diagnosis of polytrauma who were treated at the Municipal Non-Profit Enterprise “Lviv First Territorial Medical Association” of the St. Luke’s Hospital, in the anesthesiology unit with intensive care beds, from January 1, 2021 to August 1, 2022. The inclusion in the treatment of tranexamic acid on the first day after polytrauma was evaluated by dividing the obtained data into time intervals: the prehospital stage and the first 3 hours after admission; 3–8 and 8–24 hours after admission for treatment. Coagulation hemostasis was assessed by the international normalized ratio, partial thromboplastin time (PTT), level of total fibrinogen and D-dimers. The occurrence of minor bleedings was determined visually. Research stages: first day (d1), third day (d3) after polytrauma. Results. We studied indicators of coagulation hemostasis: on the first day, there is a significant increase in prothrombin time, a decrease in the prothrombin index and the level of total fibrinogen, an increase in the international normalized ratio and PTT. On the third day after injury, all studied indicators, with the exception of PTT, did not reliably differ from similar indicators of the control group. The level of D-dimers at all stages of the study was higher than normal values. After assessing the frequency of minor bleedings in patients 1–5 days after the injury, it was found that such bleedings were not associated with coagulation disorders. Conclusions. When analyzing the coagulation hemostasis, we have revealed that on the third day after injury, all indicators, except PTT, became normal. It was found that the occurrence of minor bleedings was not associated with coagulation disorders; therefore, they might be associated with vascular and platelet changes or fibrinolytic disorders.
коагулопатія; коагуляційний гемостаз; політравма
coagulopathy; coagulation hemostasis; polytrauma
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Department of Violence and Injury Prevention and Disability World Health Organization. Injuries and Violence: The Facts. [(accessed on 22 February 2020)]. http://whqlibdoc.who.int/publications/2010/9789241599375_eng.pdf.
- Frith D., Goslings J.C., Gaarder C. et al. Definition and drivers of acute traumatic coagulopathy: Clinical and experimental investigations. J. Thromb. Haemost. 2010. 8. 1919-1925. doi: 10.1111/j.1538-7836.2010.03945.x.
- Spahn D.R., Bouillon B., Cerny V. et al. The European guideline on management of major bleeding and coagulopathy following trauma: fifth edition. Crit. Care. 2019. 23. 98. https://doi.org/10.1186/s13054-019-2347-3.
- Brohi K., Singh J., Heron M., Coats T. Acute traumatic coagulopathy. J. Trauma. 2003. 54. 1127-30.
- Petros S. Trauma-Induced Coagulopathy. Hamostaseologie. 2019 Feb. 39(1). 20-27. doi: 10.1055/s-0039-1677853. Epub 2019 Jan 31. PMID: 30703820.
- Ditzel R.M. Jr et al. A review of transfusion-and trauma-induced hypocalcemia: is it time to change the lethal triad to the lethal diamond? J. Trauma Acute Care Surg. 2020. 88. 434-439.
- Rossaint R., Cerny V., Coats T.J. et al. Key issues in advanced bleeding care in trauma. Shock. 2006. 26. 322-31.
- Kornblith L.Z., Moore H.B., Cohen M.J. Trauma-induced coagulopathy: The past, present, and future. J. Thromb Haemost. 2019 Jun. 17(6). 852-862. doi: 10.1111/jth.14450. Epub 2019 May 13. PMID: 30985957; PMCID: PMC6545123.
- Sumislawski J.J., Kornblith L.Z., Conroy A.S. et al. Dynamic coagulability after injury: Is delaying venous thromboembolism chemoprophylaxis worth the wait? J. Trauma Acute Care Surg. 2018. 85. 907.
- Hess J.R., Lindell A.L., Stansbury L.G. et al. The prevalence of abnormal results of conventional coagulation tests on admission to a trauma center. Transfusion. 2009. 49(1). 34-39.
- Cohen M.J., Kutcher M., Redick B. et al.; PROMMTT Study Group. Clinical and mechanistic drivers of acute traumatic coagulopathy. J. Trauma Acute Care Surg. 2013. 75(1). Suppl. 1. S40-S47.
- Mccully S.P., Fabricant L.J., Kunio N.R. et al. The International normalized ratio overestimates coagulopathy in stable trauma and surgical patients. J. Trauma Acute Care Surg. 2013. 75. 947-53. doi: 10.1097/TA.0b013e3182a9676c.
- Hagemo J.S., Stanworth S., Juffermans N.P. et al. Prevalence, predictors and outcome of hypofibrinogenaemia in trauma: a multicentre observational study. Crit. Care. 2014. 18(2). R52.
- McQuilten Z.K., Wood E.M., Bailey M. et al. Fibrinogen is an independent predictor of mortality in major trauma patients: a five-year statewide cohort study. Injury. 2017. 48(5). 1074-1081.