
Международный неврологический журнал 4 (74) 2015
Вернуться к номеру
Impact of combination clinical, anamnestic and genetic risk factors in the development of strokes in childhood
Авторы: Smulska N. - Department of Neurology, Pediatric Hospital 1, Kiev, Ukraine
Рубрики: Неврология
Разделы: Справочник специалиста
Версия для печати
Objectives. Study combination of clinical, anamnesis and genetic risk factors (polymorphism of genes MTHFR (C677T), MTHFR (A1298C), MTRR (A66G), ACE (I/D), FII (G20210A), FV (G1691A)) in the development of strokes in childhood.
Material and methods. In this study, we analyzed data for a total of 122 patients. Children had classified into the groups. Main group included children with ischemic stroke (n=47) and hemorrhagic stroke (n=31) and control group (n=44). All patients had investigated in the Neurology Department between January 2009 and December 2013. All children in the main group had acute stroke with clinically and radiologically confirmed. In control group were enrolled healthy children. All patients (in main and control groups) were between 0 days and 14th years and 11 months old.
We had analyses anamnesis of children: problems before and along pregnancy (anemia, pressure, mother’s illnesses), taking vitamins, gestosis, delivery (normal, abnormal), the age of gestation, weight, height, Apgar score, reanimation in the neonatal period, family anamnesis (strokes in the families). In the main group we had the more frequency reanimation in the neonatal period, Apgar score ≤ 6, weight in the newborn period ≤ 2500 and height ≤ 49 cm in the anamsesis.
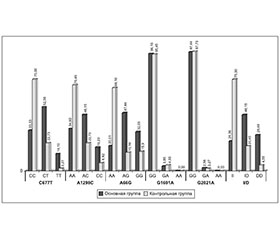
All patients had genetics investigation - polymorphism of genes MTHFR (C677T), MTHFR (A1298C), MTRR (A66G), ACE (I/D), FII (G20210A), FV (G1691A). We had not any statistically defenses of polymorphism genes FII (G20210A), FV (G1691A) in the main group and control group. Therefore, we included in the study polymorphism of genes MTHFR (C677T), MTHFR (A1298C), MTRR (A66G), ACE (I/D). We saw authentic increase frequency polymorphism СТ of MTHFR_С677Т gene (χ2=9,10, р<0,003, OR=3,77 95%CI:1,64-8,67), polymorphism АС of gene MTHFR_A1298C (χ2=5,61 р<0,018, OR=2,91 95%CI:1,27-6,71), polymorphism AG of gene MTRR_A66G (χ2 = 4,01 р<0,045, OR=2,80 95%CI: 1,10-7,11), polymorphism ID (χ2 = 6,92 р< 0,009, OR=3,33 95%CI: 1,41-7,86) and DD of gene АСЕ (χ2 = 9,26 р< 0,002, OR=8,78 95%CI: 1,96-39,35) in the main group comparison with group of control.
Results. At first, we study the best prognostic model for risk factors in group of children with strokes (ischemic and hemorrhagic) (we use MDR method). The model included age of gestation/ reanimation in the newborn period/ polymorphism ACE_I/D with 100% reproducibility and accuracy of prediction of was 91,96%. Next, we researched prognostic model separately for IS and HS. The best prognostic model in the development of ischemic stroke in childhood included gestation age, problems in newborn period (reanimation) and C677T polymorphism MTHFR genе – accuracy of prediction was 82,78%. In the group of children with hemorrhagic stroke the best prognostic model included three factors: the age of gestations, A66G polymorphism of MTRR genе and I/D polymorphism of ACE genе - accuracy of prediction was 74,23%/.
Then, we study influence of genetic polymorphism for the age of acute stroke. The middle of age children in our investigation was 44,01±7,01 months. In group of IS the early debut was associations with DD genotype of ACE gene (15,33±4,31 months) and GG genotype of MTRR gene (28,50±4,82months); more frequency genotype 1298CC and 677TT of MTHFR gene we saw in the older group (debut in 49,25±13,11 months and 55,26±25,5 months accordingly).
In the group of HS influents on age of debut had polymorphism of MTRR and ACE genes. DD genotype of ACE gene associations with early debut of HS - 21,05±10,12 months and GG genotype of MTRR gene - 21,89±9.97 months. We had not statistically difference between debut of HS and polymorphism of MTHFR gene.
Next, we analyses polymorphism of genes in the age’s groups between children with strokes. In our investigations we were segregation all children with strokes (78 patients) into the age: we had 14 children in group 0-28 days (17,95%), 28 children (35,89%) had age 29 days – 1 year, 18 children (23,08%) was in group 1 year 1 day – 6 years, and the same group include children from 6 years 1 day to 14 years 11 months . In group of children 0-28 days the more frequency we saw polymorphism of ACE, MTHFR (С677Т), MTRR genes, in group 29 days – 1 year – polymorphism of MTHFR (С677Т) gene, in group older than 6 years – polymorphism MTRR (A66G). Children with IS and HS in the youngest group had DD genotype ACE gene (p<0,001) and GG genotype MTRR gene (p<0,005).
In the end, we study family anamnesis. 28 children (59,57±7,15%) in group of IS had a cases of strokes in family. In the control group 5 children (11,36 ±4,78%) had families strokes.
Conclusions.