
Международный эндокринологический журнал Том 19, №8, 2023
Вернуться к номеру
Вплив цукрового діабету 2-го типу на серцеву недостатність зі збереженою фракцією викиду залежно від наявності фібриляції передсердь
Авторы: N.M. Kulaiets, V.M. Kulaiets, O.O. Tkachuk-Hryhorchuk, N.B. Nyshchuk-Oliinyk
Ivano-Frankivsk National Medical University, Ivano-Frankivsk, Ukraine
Рубрики: Эндокринология
Разделы: Клинические исследования
Версия для печати
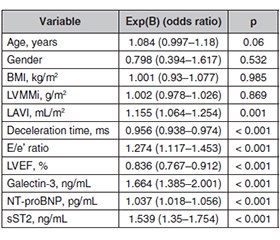
Актуальність. Серцево-судинні захворювання, включаючи серцеву недостатність (СН) та серцеву недостатність зі збереженою фракцією викиду (СНзбФВ), є глобальною проблемою охорони здоров’я. Захворюваність на СН зі збереженою фракцією викиду зростає, особливо серед людей похилого віку та тих, хто страждає на діабет, ожиріння та гіпертензію. Цукровий діабет 2-го типу (ЦД2) часто співіснує з СНзбФВ, а фібриляція передсердь (ФП) ще більше ускладнює ситуацію через спільні фактори ризику. Мета дослідження: комплексно вивчити вплив ЦД2 на серцеву функцію та біомаркерні профілі в пацієнтів із СН зі збереженою фракцією викиду за наявності або відсутності фібриляції передсердь. Матеріали та методи. Дослідження було когортним одноцентровим. Обстежено 448 пацієнтів із СНзбФВ. Вони були розподілені на 4 групи: перша група — 189 осіб лише з СНзбФВ; друга група — 39 пацієнтів із СНзбФВ та ЦД2; третя група — 176 хворих із СНзбФВ та фібриляцією передсердь; четверта група — 44 пацієнти з СНзбФВ, ФП, ЦД2. Результати. ЦД2 сам по собі суттєво не впливає на індекс маси лівого шлуночка, але в поєднанні з ФП впливає. ЦД2 асоціюється зі збільшенням індексу об’єму лівого передсердя, а ФП посилює цей ефект. Діабет впливає на діастолічну функцію, а ФП погіршує її. ЦД2 впливає на тиск наповнення лівого шлуночка, а ФП погіршує його при СНзбФВ. ЦД2 також впливає на систолічну функцію лівого шлуночка, яка погіршується при поєднанні з ФП в осіб із СНзбФВ. Рівень галектину-3 підвищений у пацієнтів із СНзбФВ на тлі ЦД2, що ще більше посилюється за наявності ФП. Уміст NT-proBNP залежить від діабету й погіршується при поєднанні з ФП в осіб із СНзбФВ. Рівень sST2 підвищений у хворих на СНзбФВ із ЦД2 та ще більше підвищується при поєднанні з ФП, що вказує на фіброз міокарда й несприятливе ремоделювання. Висновки. Взаємодія ЦД2 та ФП у пацієнтів із СНзбФВ створює синергічний ефект, що призводить до значних структурних і функціональних змін серця. Нові біомаркери, такі як галектин-3, NT-proBNP і sST2, є цінними діагностичними інструментами, що відображають складні патофізіологічні процеси при СНзбФВ.
Background. Cardiovascular diseases, including heart failure (HF) and heart failure with preserved ejection fraction (HFpEF), pose a global health challenge. HFpEF is on the rise, especially among the elderly and those with conditions like diabetes, obesity, and hypertension. Type 2 diabetes mellitus (T2DM) often coexists with HFpEF, and atrial fibrillation (AF) further complicates matters due to shared risk factors. The purpose of this study is to comprehensively investigate the influence of type 2 diabetes mellitus on cardiac function and biomarker profiles in patients with heart failure with preserved ejection fraction in the presence or absence of atrial fibrillation. Materials and methods. This was a cohort, single-center study. Four hundred and forty-eight patients with HFpEF were examined. They were divided into 4 groups: group 1 — 189 patients with HFpEF alone; group 2 — 39 patients with HFpEF and T2DM; group 3 — 176 patients with HFpEF and atrial fibrillation; group 4 — 44 patients with HFpEF, AF, T2DM. Results. T2DM may contribute to a slightly older patient population in HFpEF, but age alone is not a primary discriminator. T2DM alone does not substantially impact left ventricular mass index but, when combined with AF, it does. T2DM is associated with an increased left atrial volume index, and AF intensifies this effect. T2DM influences diastolic function, with AF exacerbating it. T2DM affects left ventricular filling pressure, and AF worsens this in HFpEF. T2DM also influences left ventricular systolic function, further compromised when combined with AF in HFpEF patients. Galectin-3 levels are elevated in HFpEF patients with T2DM, further exacerbated with AF. NT-proBNP levels are influenced by T2DM and worsened with the combination of AF in HFpEF. SST2 levels are elevated in HFpEF patients with T2DM, further increased with AF, indicating myocardial fibrosis and adverse remodeling. Conclusions. The interaction between T2DM and AF in HFpEF patients creates a synergistic effect, resulting in significant cardiac structural and functional alterations. Novel biomarkers such as galectin-3, NT-proBNP, and sST2 emerge as valuable diagnostic tools, reflecting the complex pathophysiological processes in HFpEF.
цукровий діабет; лівий шлуночок; діастолічна дисфункція; серцева недостатність зі збереженою фракцією викиду; фібриляція передсердь
diabetes mellitus; left ventricle; diastolic dysfunction; heart failure with preserved ejection fraction; atrial fibrillation
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Redfield M.M., Borlaug B.A. Heart Failure with Preserved Ejection Fraction: A Review. JAMA. 2023. 329(10). 827-38. doi: 10.1001/JAMA.2023.2020.
- Iyngkaran P., Thomas M.C., Neil C., Jelinek M., Cooper M., Horowitz J.D. et al. The Heart Failure with Preserved Ejection Fraction Conundrum — Redefining the Problem and Finding Common Ground? Curr. Heart Fail. Rep. 2020. 17(2). 34-42. doi: 10.1007/S11897-020-00454-2.
- McHugh K., DeVore A.D., Wu J., Matsouaka R.A., Fona–row G.C., Heidenreich P.A. et al. Heart Failure with Preserved Ejection Fraction and Diabetes: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2019. 73(5). 602-11. doi: 10.1016/J.JACC.2018.11.033.
- Lejeune S., Roy C., Slimani A., Pasquet A., Vancraeynest D., Vanoverschelde J.L. et al. Diabetic phenotype and prognosis of patients with heart failure and preserved ejection fraction in a real life cohort. Cardiovasc. Diabetol. 2021. 20(1). 1-12. doi: 10.1186/S12933-021-01242-5.
- Obokata M., Reddy Y.N.V., Borlaug B.A. Diastolic Dysfunction and Heart Failure with Preserved Ejection Fraction: Understanding Mechanisms by Using Noninvasive Methods. JACC Cardiovasc. Ima–ging. 2020. 13(1). 245-57. doi: 10.1016/J.JCMG.2018.12.034.
- Reddy Y.N.V., Obokata M., Verbrugge F.H., Lin G., Borlaug B.A. Atrial Dysfunction in Patients with Heart Failure with Preserved Ejection Fraction and Atrial Fibrillation. J. Am. Coll. Cardiol. 2020. 76(9). 1051-64. doi: 10.1016/J.JACC.2020.07.009.
- Gulsin G.S., Kanagala P., Chan D.C.S., Cheng A.S.H., Athithan L., Graham-Brown M.P.M. et al. Differential left ventricular and left atrial remodelling in heart failure with preserved ejection fraction patients with and without diabetes. Ther. Adv. Endocrinol. Metab. 2019. 10. doi: 10.1177/2042018819861593.
- Yap J., Tay W.T., Teng T.H.K., Anand I., Richards A.M., Ling L.H. et al. Association of diabetes mellitus on cardiac remode–ling, quality of life, and clinical outcomes in heart failure with reduced and preserved ejection fraction. J. Am. Heart Assoc. 2019. 8(17). doi: 10.1161/JAHA.119.013114.
- Liu G., Long M., Hu X., Hu C.H., Du Z.M. Meta-Analysis of Atrial Fibrillation and Outcomes in Patients with Heart Failure and Preserved Ejection Fraction. Heart Lung Circ. 2021. 30(5). 698-706. doi: 10.1016/j.hlc.2020.10.010.
- Merino-Merino A., Saez-Maleta R., Salgado-Aranda R., AlKassam-Martinez D., Pascual-Tejerina V., Martin-Gonzalez J. et al. Biomarkers in atrial fibrillation and heart failure with non-reduced ejection fraction: Diagnostic application and new cut-off points. Heart & Lung. 2020. 49(4). 388-92. doi: 10.1016/j.hrtlng.2020.02.043.
- Yan X., Guo Y., Li L., Wang Z., Li Z. The sST2 level is an independent influencing factor associated with atrial fibrillation in heart failure patients: a case-control study. J. Thorac. Dis. 2022. 14(5). 1578-87. doi: 10.21037/JTD-22-470/COIF.
- Li M., Duan L., Cai Y., Hao B., Chen J., Li H. et al. Prognostic value of soluble suppression of tumorigenesis-2 (sST2) for cardiovascular events in coronary artery disease patients with and without diabetes mellitus. Cardiovasc. Diabetol. 2021. 20(1). 1-11. doi: 10.1186/S12933-021-01244-3.
- Hara A., Niwa M., Kanayama T., Noguchi K., Niwa A., Matsuo M. et al. Galectin-3: A Potential Prognostic and Diagnostic Marker for Heart Disease and Detection of Early Stage Pathology. Biomolecules. 2020. 10(9). 1277. doi: 10.3390/BIOM10091277.
- Schmitt V.H., Prochaska J.H., Föll A.S., Schulz A., Keller K., Hahad O. et al. Galectin-3 for prediction of cardiac function compared to NT-proBNP in individuals with prediabetes and type 2 diabetes mellitus. Scientific Reports. 2021. 11(1). 1-12. doi: 10.1038/s41598-021-98227-x.
- Bertoni M., Bini C., Bracciali A. Galectin-3 in Heart Failure with Preserved Ejection Fraction and Persistent Atrial Fibrillation Versus Sinus Rhythm. Correlation with Left Atrial Volume and N-Terminal Pro B-Type Natriuretic Peptide. J. Cardiovasc. Disord. 2021. 7(1). 1043. doi: 10.26420/jcardiovascdisord.2021.1043.
- Ponikowski P., Voors A.A., Anker S.D., Bueno H., Cleland J.G.F., Coats A.J.S. et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail. 2016. 18(8). 891-975. doi: 10.1002/EJHF.592.
- Hindricks G., Potpara T., Dagres N., Arbelo E., Bax J.J., Blomström-Lundqvist C. et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2021. 42(5). 373-498. doi: 10.1093/eurheartj/ehaa612.
- Cosentino F., Grant P.J., Aboyans V., Bailey C.J., Ceriello A., Delgado V. et al. 2019 ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD: The Task Force for diabetes, pre-diabetes, and cardiovascular diseases of the European Society of Cardiology (ESC) and the European Asso–ciation for the Study of Diabetes (EASD). Eur. Heart J. 2020. 41(2). 255-323. doi: 10.1093/eurheartj/ehz486.
- Lang R.M., Badano L.P., Mor-Avi V., Afilalo J., Armstrong A., Ernande L. et al. Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Journal of the American Society of Echocardiography. 2015. 28(1). 1-39.e14. doi: 10.1016/j.echo.2014.10.003.
- Nagueh S.F., Smiseth O.A., Appleton C.P., Byrd B.F., Dokainish H., Edvardsen T. et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Journal of the American Society of Echocardiography. 2016. 29(4). 277-314. doi: 10.1016/j.echo.2016.01.011.
- Shang Y., Zhang X., Leng W., Lei X., Chen L., Zhou X. et al. Increased fractal dimension of left ventricular trabeculations is associated with subclinical diastolic dysfunction in patients with type-2 diabetes mellitus. International Journal of Cardiovascular Imaging. 2019. 35(4). 665-73. doi: 10.1007/S10554-018-1492-0.
- Sartipy U., Dahlström U., Fu M., Lund L.H. Atrial Fibrillation in Heart Failure with Preserved, Mid-Range, and Reduced Ejection Fraction. JACC Heart Fail. 2017. 5(8). 565-74. doi: 10.1016/J.JCHF.2017.05.001.
- Lam C.S.P., Rienstra M., Tay W.T., Liu L.C.Y., Hummel Y.M., van der Meer P. et al. Atrial Fibrillation in Heart Failure with Preserved Ejection Fraction: Association with Exercise Capacity, Left Ventricular Filling Pressures, Natriuretic Peptides, and Left Atrial Volume. JACC Heart Fail. 2017. 15(1). 19-24. doi: 10.1016/J.JCHF.2016.10.005.
- Jasic-Szpak E., Marwick T.H., Donal E., Przewlocka-Kosmala M., Huynh Q., Gozdzik A. et al. Prediction of AF in Heart Failure with Preserved Ejection Fraction: Incremental Value of Left Atrial Strain. Cardiovascular Imaging. 2021. 14(1). 131-44. doi: 10.1016/J.JCMG.2020.07.040.
- O’Neal W.T., Sandesara P., Patel N., Venkatesh S., Samman-Tahhan A., Hammadah M. et al. Echocardiographic predictors of atrial fibrillation in patients with heart failure with preserved ejection fraction. Eur. Heart J. Cardiovasc. Imaging. 2017. 18(7). 725-9. doi: 10.1093/EHJCI/JEX038.
- Inciardi R.M., Claggett B., Gupta D.K., Cheng S., Liu J., Tcheugui J.B.E. et al. Cardiac Structure and Function and Diabetes-Related Risk of Death or Heart Failure in Older Adults. J. Am. Heart Assoc. 2022. 11(6). 22308. doi: 10.1161/JAHA.121.022308.
- Bouthoorn S., Valstar G.B., Gohar A., den Ruijter H.M., Reitsma H.B., Hoes A.W. et al. The prevalence of left ventricular diastolic dysfunction and heart failure with preserved ejection fraction in men and women with type 2 diabetes: A systematic review and meta-analysis. Diab. Vasc. Dis. Res. 2018. 15(6). 477-93. doi: 10.1177/1479164118787415.
- Kristensen S.L., Mogensen U.M., Jhund P.S., Petrie M.C., Preiss D., Win S. et al. Clinical and Echocardiographic Characte–ristics and Cardiovascular Outcomes According to Diabetes Status in Patients with Heart Failure and Preserved Ejection Fraction: A Report from the I-Preserve Trial (Irbesartan in Heart Failure with Preserved Ejection Fraction). Circulation. 2017. 135(8). 724-35. doi: 10.1161/CIRCULATIONAHA.116.024593.
- Herashchenko A.S., Fedorov S.V., Bielinskyi M.V., Sere–dyuk N.M., Kozlova I.V. Predicting heart failure in patients with diabetes mellitus: galectin-3, SST2, and carotid thickness. World of Medicine and Biology. 2023. 19(84). 45. doi: 10.26724/2079-8334-2023-2-84-45-49.
- Puri D., Kaur J., Gaur N., Kodidala S.R. Role of glycated hemoglobin in microvascular complications in type 2 diabetes mellitus: cross sectional study. International Journal of Endocrinology (Ukraine). 2022. 18(6). 319-323. doi: 10.22141/2224-0721.18.6.2022.1201.
- Koval S.M., Yushko K.O., Snihurska I.O., Starchenko T.G., Pankiv V.I., Lytvynova O.M., Mysnychenko O.V. Relations of angiotensin-(1-7) with hemodynamic and cardiac structural and functional parameters in patients with hypertension and type 2 diabetes. Arterial Hypertension. 2019. 23(3). 183-189. doi: 10.5603/AH.a2019.0012.