
Журнал «Травма» Том 24, №3, 2023
Вернуться к номеру
Біомеханічне обґрунтування алгоритму вибору варіанта коригуючої остеотомії V плеснової кістки в лікуванні деформації Тейлора
Авторы: Прозоровський Д.В., Златник Р.В., Карпінський М.Ю., Карпінська О.Д.
ДУ «Інститут патології хребта та суглобів ім. проф. М.І. Ситенка НАМН України», м. Харків, Україна
Рубрики: Травматология и ортопедия
Разделы: Клинические исследования
Версия для печати
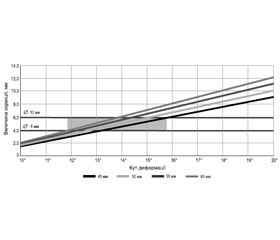
Актуальність. Деформацію суглоба між основною фалангою 5-го пальця стопи та V плесновою кісткою прийнято називати деформацією Тейлора. Лікування деформації Тейлора найчастіше хірургічне. При цьому відзначається відсутність єдиного підходу щодо застосування остеотомій, їх виду та локалізації на плесновій кістці (дистальні, діафізарні та проксимальні). Мета: на підставі біомеханічних досліджень обґрунтувати коригувальні можливості дистальних остеотомій Weil та Shevron для усунення вальгусної деформації V плеснової кістки залежно від її геометричних параметрів. Матеріали та методи. Моделювали два варіанти коригувальних остеотомій: остеотомія Weil та остеотомія Shevron. Визначали максимально можливі величини вальгусної деформації V плеснової кістки, які можуть бути усунені за допомогою цих остеотомій залежно від геометричних параметрів V плеснової кістки. Для визначення геометричних параметрів V плеснової кістки проводили рентгенометрію за 39 цифровими рентгенограмами стоп пацієнтів. Результат. З огляду на відносне невелике кутове відхилення V плеснової кістки, величина якого найчастіше спостерігається в межах від 10 до 15° при нормі 8°, кутову деформацію можна компенсувати лінійним зміщенням головки плеснової кістки. Оскільки зміщення головки виконують у горизонтальній площині, обидві остеотомії у даному випадку працюють абсолютно однаково. Зона максимально можливої корекції деформацій визначається в межах від 12° при довжині 60 мм і діаметрі 8 мм до 15,5° при довжині 45 мм і діаметрі 12 мм. З урахуванням того, що існує якийсь баланс між довжиною та діаметром кістки, можна вважати максимальною деформацією, яку можна усунути за допомогою коригувальних остеотомій Weil та Shevron, деформацію до 14°. Висновки. Коригувальні остеотомії Weil та Shevron можуть бути застосовані для корекції вальгусної деформації V плеснової кістки (деформації Тейлора) та ефективні в використанні при куті M4M5, який не перевищує показник в 14°. У тих випадках, коли кут M4M5 перевищує показник 15°, доцільно використовувати проксимальні коригувальні остеотомії V плеснової кістки при лікуванні деформації Тейлора.
Background. Joint deformity between the main phalanx of the fifth toe and the fifth metatarsal bone is called tailor’s bunion. Its treatment is most often surgical. At the same time, there is no unified single approach regarding the use of osteotomies, their type and localization on the metatarsal bone (distal, diaphyseal, and proximal). Goal: based on the biomechanical studies, to substantiate the corrective possibilities of Weil and chevron distal osteotomies to correct valgus deformity of the fifth metatarsal bone depending on its geometric parameters. Materials and methods. Two types of corrective osteotomies were modeled: Weil and chevron osteotomy. We determined the maximum possible values of valgus deformity of the fifth metatarsal bone, which can be eliminated with the help of these osteotomies, depending on the geometric parameters of the fifth metatarsal bone. To determine the latter, radiometry was performed on 39 digital radiographs of the patients’ feet. Results. Taking into account the relatively small angular deviation of the fifth metatarsal bone whose value is most often observed in the range from 10 to 15° at the norm of 8°, the angular deformity can be compensated by linear displacement of the head of the metatarsal bone. Since the head displacement is performed in the horizontal plane, both osteotomies in this case work equally. The zone of maximum possible correction for deformity is determined within the range from 12°, with a length of 60 mm and a diameter of 8 mm, to 15.5°, with a length of 45 mm and a diameter of 12 mm. Given that there is some balance between bone length and diameter, the maximum deformity that can be corrected with Weil and chevron corrective osteotomies is a deformity of up to 14°. Conclusions. Weil and chevron corrective osteotomies can be used to correct the fifth metatarsal valgus deformity (tailor’s bunion) and are effective when the M4M5 angle does not exceed 14°. In cases where the M4M5 angle exceeds 15°, it is advisable to use proximal corrective osteotomies of the fifth metatarsal bone for the treatment of tailor’s bunion.
стопа; деформація; остеотомія
foot; deformity; osteotomy