
Журнал «Почки» Том 12, №2, 2023
Вернуться к номеру
Глюкокортикоїди в лікуванні IgA-нефропатії: за і проти. Дані досліджень і власний досвід
Авторы: Чуб О.І.
ННІ післядипломної освіти Харківського національного медичного університету, м. Харків, Україна
Рубрики: Нефрология
Разделы: Справочник специалиста
Версия для печати
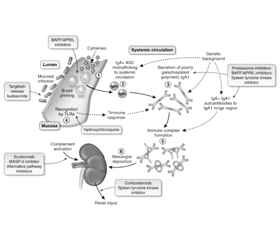
IgA-нефропатія є найбільш поширеним патерном первинних гломерулярних захворювань у всьому світі. Клінічні прояви варіюють від ізольованої гематурії до нефротичної протеїнурії, гострого ураження нирок і хронічної хвороби нирок. 10-річний ризик прогресування IgA-нефропатії до термінальної ХХН становить 26 %. Основою лікування IgA-нефропатії є цілеспрямована підтримуюча терапія, що включає: оптимізацію контролю артеріального тиску, використання блокаторів ренін-ангіотензинової системи в максимально переносимих дозах; нову групу препаратів — інгібітори натрій-залежного котранспортера глюкози; модифікацію способу життя, що передбачає відмову від паління, контроль ваги й обмеження споживання натрію. Проте супортивна терапія не завжди досягає своїх цілей і не може вплинути на автоімунний патогенез захворювання. Тоді як роль імунодепресантів і системних глюкокортикостероїдів залишається суперечливою. У цьому огляді подано аналіз клінічних досліджень і власний досвід щодо ролі стероїдів і супортивної терапії в лікуванні IgA-нефропатії.
IgA nephropathy is the most common pattern of primary glomerular diseases worldwide and remains a leading cause of chronic kidney disease and kidney failure. The incidence of IgA nephropathy is 2.5 per 100,000 population per year. Presentation ranges from isolated haematuria to significant proteinuria, acute kidney injury and even chronic kidney disease. The 10-year risk of progression to end stage kidney disease or halving of GFR is 26 %. The basis of management of IgA nephropathy is goal-directed supportive care in the form of rigorous blood pressure control, use of renin-angiotensin system blockers in the maximum tolerated dose, and a focus on life-style modification that includes smoking cessation, weight management, and restriction of sodium intake. However, supportive therapy does not always achieve its goals and cannot affect the autoimmune pathogenesis of the disease, while the role of immunosuppressants and systemic glucocorticoids remains controversial. This review presents an analysis of clinical trials and our own experience regarding the role of steroids and supportive therapy in the treatment of IgA nephropathy.
IgA-нефропатія; глюкокортикоїди; інгібітори ренін-ангіотензинової системи; інгібітори натрій-залежного котранспортера глюкози; лікування; протеїнурія; розрахункова швидкість клубочкової фільтрації; хронічна хвороба нирок
IgA nephropathy; glucocorticoids; renin-angiotensin system inhibitors; sodium-glucose cotransporter-2 inhibitors; treatment; proteinuria; estimated glomerular filtration rate; chronic kidney disease
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Rodrigues J.C., Haas M., Reich H.N. IgA Nephropathy. Clin. J. Am. Soc. Nephrol. 2017. 12(4). 677-86. https://doi.org/10.2215/CJN.07420716; PMID: 28159829.
- Coppo R., Troyanov S., Bellur S., Cattran D., Cook H.T., Feehally J. et al. Validation of the Oxford classification of IgA nephropathy in cohorts with different presentations and treatments. Kidney Int. 2014. 86(4). 828-36. https://doi.org/10.1038/ki.2014.63; PMID: 24694989.
- Cheung C.K., Barratt J. Further Evidence for the Mucosal Origin of Pathogenic IgA in IgA Nephropathy. JASN. 2022. 33(5). Р. 873-875. DOI: 10.1681/ASN.2022020201.
- Floege J. et al. Current treatment of IgA nephropathy. Seminars in Immunopathology. 2021. 43. 717-728: https://doi.org/10.1007/s00281-021-00888-3.
- KDIGO 2021 Clinical Practice Guideline for the Management of Glomerular Diseases.
- Zhang Y.-M. et al. Glucocorticoids for IgA nephropathy — pro. Kidney International. 2023. 103. 666-669. https://doi.org/10.1016/j.kint.2023.01.018.
- Lv J. et al. Corticosteroid Therapy in IgA Nephropathy. J. Am. Soc. Nephrol. 2012 Jun. 23(6). 1108-1116. doi: 10.1681/ASN.2011111112.
- Manno С. et al. Randomized controlled clinical trial of corticosteroids plus ACE-inhibitors with long-term follow-up in proteinuric IgA nephropathy. Nephrology Dialysis Transplantation. 2009. Vol. 24. Issue 12. P. 3694-3701. https://doi.org/10.1093/ndt/gfp356.
- Lv J. et al. Combination Therapy of Prednisone and ACE Inhibitor Versus ACE-Inhibitor Therapy Alone in Patients With IgA Nephropathy: A Randomized Controlled Trial. American Journal of Kidney Diseases. 2009. Vol. 53. Issue 1. P. 26-32. https://doi.org/10.1053/j.ajkd.2008.07.029.
- Rauen Т. et al. After ten years of follow-up, no difference between supportive care plus immunosuppression and supportive care alone in IgA nephropathy. Kidney International. 2020. Vol. 98. Issue 4. P. 1044-1052. https://doi.org/10.1016/j.kint.2020.04.046.
- Rauen Т. et al. Intensive Supportive Care plus Immunosuppression in IgA Nephropathy. N. Engl. J. Med. 2015. 373. 2225-2236. N. Engl. J. Med. 2015. 373. 2225-2236. DOI: 10.1056/NEJMoa1415463.
- Cheung C.K., Barratt J. First do no harm: systemic glucocorticoids should not be used for the treatment of progressive IgA nephropathy. Kidney International. 2023. 103. 669-673. https://doi.org/ 10.1016/j.kint.2022.05.034.
- Rovin B.H. IgA nephropathy and glucocorticoids — a limbo dance? Kidney International. 2023. 103. 673. https://doi.org/ 10.1016/j.kint.2023.01.017.
- Cheung C.K. et al. An Update on the Current State of Management and Clinical Trials for IgA Nephropathy. J. Clin. Med. 2021 Jun. 10(11). 2493. doi: 10.3390/jcm10112493.
- Floege J. еt al. Management and Treatment of Glomerular Diseases (Part 1): Conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int. 2019. 95. 268-280. doi: 10.1016/j.kint.2018.10.018.