Вступ
Регматогенне відшарування сітківки (РВС) — одне з найскладніших захворювань органа зору, суть якого полягає у відокремленні нейросенсорної сітківки від комплексу пігментного епітелію та мембрани Бруха, накопиченні рідини між цими шарами та наявності розриву сітківки [1, 2]. РВС займає частку від 2 до 9 % у структурі первинної інвалідності із захворювань органа зору [3, 4]. При проведенні епідеміологічних спостережень поширеність РВС у світовому масштабі, за даними деяких авторів, становить 10–18 випадків, за даними інших — 6,9–18,2 випадку на 100 000 населення на рік [5, 6]. У країнах Європи цей показник становить 6–10 випадків на 100 000 населення на рік [1].
Доведено, що частота виникнення цього захворювання серед чоловіків вища, ніж серед жінок, пік захворюваності припадає на 20–29 років (8 випадків на 100 000 населення) та 60–70 років (28 випадків на 100 000 населення). Протягом першого року ризик розвитку РВС на парному оці підвищується на 3,5–5,8 %, а у наступні чотири роки — на 9–10 % [1, 2, 7, 8].
За даними різних авторів, ефективність хірургії широко варіює незалежно від обраного методу лікування та знаходиться в межах від 37 до 95 % [9]. Отже, на сьогодні існує три групи патогенетично орієнтованих оперативних втручань: екстраокулярні, інтраокулярні та комбіновані. Вибір методу лікування РВС має бути індивідуальним у кожному клінічному випадку; лікар має брати до уваги вік пацієнта, тривалість існування відшарування, його характер, вид та площу, рухомість відшарованої сітківки, стадію проліферативної вітреоретинопатії та наявність в анамнезі оперативних втручань [10]. У низці випадків виконується закрита субтотальна вітректомія (ЗСВ) з наступною тампонадою вітреальної порожнини газоповітряною сумішшю та ендолазеркоагуляцією. Окрім газів, для стабілізації положення сітківки та її прилягання використовують важкі рідини — перфторорганічні сполуки або силіконове масло, які, у свою чергу, дозволяють контролювати інтраопераційні маніпуляції на сітківці та можуть знаходитися у вітреальній порожнині більш тривалий період [11].
Кожен з методів має свої переваги та недоліки, але мініінвазивність ендовітреальної хірургії, краща візуалізація деталей заднього полюса ока, удосконалення фізико-хімічних властивостей тампонуючих речовин сприяє вибору закритої субтотальної вітректомії як першої ланки лікування РВС [12].
Виконання закритої субтотальної вітректомії на факічних очах нерідко призводить до розвитку або прогресування катаракти; за даними літератури, її частота становить від 20 до 80 %. Це призводить до зниження зорових функцій і, як наслідок, до погіршення якості життя цієї категорії пацієнтів. Поєднання факоемульсифікації катаракти (ФЕК) та закритої субтотальної вітректомії має безсумнівні переваги, а саме: поліпшує візуалізацію структур ока під час операції і після неї, дає можливість більш ефективно впливати на післяопераційну рефракцію ока, забезпечує повне видалення склоподібного тіла без пошкодження кришталика, скорочує кількість хірургічних втручань, знижує анестезіологічне навантаження [13].
Мета — вивчити ефективність сучасних методів комбінованого хірургічного лікування регматогенного відшарування сітківки і вікової катаракти.
Матеріали та методи
Під спостереженням знаходилося 60 пацієнтів (60 очей) із регматогенним відшаруванням сітківки у поєднанні з віковою катарактою, яким виконували закриту субтотальну вітректомію з тампонадою вітреальної порожнини газоповітряною сумішшю 20% C3F8, ендолазеркоагуляцією сітківки та ФЕК з імплантацією інтраокулярної лінзи (ІОЛ).
Клінічні дослідження виконували відповідно до біоетичних вимог Гельсінської декларації, прийнятої Генеральною асамблеєю Всесвітньої медичної асоціації, Конвенції Ради Європи про права людини та біомедицину (1977 р.), відповідного положення Всесвітньої організації охорони здоров’я, Міжнародної ради медичних наукових товариств, Міжнародного кодексу медичної етики (1983 р.) і законів України та наказу Міністерства охорони здоров’я України від 23.09.2009 р. № 690. Пацієнти, дані яких використовували у дисертаційному дослідженні, давали інформовану згоду.
Пацієнтам виконували субтенонову анестезію бупівакаїном 4 мл. Обробляли операційне поле розчином бетадину. Встановлювали блефаростат. За допомогою троакарів 25 G проводили встановлення портів у нижньотемпоральному, верхньоназальному та верхньотемпоральному секторах в 3,5 мм від лімба. Встановлювали іригаційну канюлю в нижньотемпоральному секторі. Проводили тунельний розріз рогівки, парацентез на 3 годинах. У передню камеру вводили віскоеластик за soft-shell технікою. Виконували капсулорексис, гідродисекцію. Проводили ультразвукове дроблення ядра з використанням іригаційного розчину. Вимивали кришталикові маси. У капсульний мішок імплантували ІОЛ SN60WF. Проводили гідратацію рогівки. Виконували закриту субтотальну вітректомію. Видаляли задню гіалоїдну мембрану. Проводили склерокомпресію та усували тракційні компоненти із мобілізацією сітківки. Ендолазерним зондом 25 G виконували ендолазеркоагуляцію виключно в місцях тракцій чи розривів із подальшою заміною рідини на стерильне повітря. У вітреальну порожнину вводили газоповітряну суміш 20% С3F8. Видаляли троакари та герметизували порти. Під кон’юнктиву вводили розчин глюкокортикостероїду. Проводили інстиляції антибіотика та накладали монокулярну асептичну пов’язку. За відсутності повної адекватної газоповітряної тампонади, при дінамічному спостереженні упродовж 1 місяця проводили додаткову заміну внутрішньоочної рідини на газоповітряну суміш в умовах операційної. Проводили епібульбарну анестезію розчином алкаїну 1%. Обробляли операційне поле водним розчином бетадину. У 3,5 мм від лімба на 5/7 годинах голкою 29 G із шприцом 10,0 з 18% газоповітряною сумішшю C3F8 сидячи проводили пункцію склери. Проводили поступову заміну рідини на стерильну 20% газоповітряну суміш до повної тампонади під візуальним контролем за допомогою налобного офтальмоскопа.
Пацієнтам у післяопераційному періоді проводили дослідження гостроти зору, внутрішньоочного тиску, периметрію Humphrey, дослідження поля зору за скринінговими тестами, оптичну когерентну томографію сітківки та зорового нерва.
Наявність у вітреальній порожнині газоповітряної суміші не дозволяла провести в ранньому післяопераційному періоді периметрію Humphrey, оптичну когерентну томографію сітківки та зорового нерва. Дослідження полів зору виконували за скринінговими тестами.
Строк спостереження — 1 рік.
Для подання кількісних показників розраховувалося середнє значення змінної (М), стандартна помилка (± m). Для визначення статистичної значущості відмінностей середніх значень у двох незалежних групах використовували t-критерій Стьюдента. Для порівняння структури груп у відсотках (P ± m) у різні терміни спостереження використовували метод арксинус-перетворення Фішера. Нульову гіпотезу про відсутність ефекту відкидали і відмінності між показниками вважали статистично значущими при рівні значущості р < 0,05.
Результати
При огляді 60 пацієнтів (60 очей) до оперативного втручання максимально коригована гострота зору 0,05–0,3 була на 22 очах (36,67 %), 0,4–0,6 — на 21 оці (35,0 %), 0,7–1,0 — на 17 очах (28,33 %) і в середньому становила 0,31 ± 0,04 (від 0,05 до 1,0). Некоригована гострота зору в середньому становила 0,18 ± 0,03. Рівень внутрішньоочного тиску в середньому був 15,5 ± 5,3 мм рт.ст.
Середній показник світлочутливості сітківки (MD) при периметрії Humphrey становив 6,14 ± 0,15 dB. Показник суми локальних дефектів полів зору (PSD) становив 4,3 ± 0,1. При дослідженні поля зору за скринінговими тестами нормальні межі поля зору були на 7 очах (11,67 %), мінімальні зміни в полі зору у вигляді відносних парацентральних скотом були на 23 очах (38,33 %), звуження поля зору на 5–10° у поєднанні з відносними скотомами — на 20 очах (33,33 %), звуження поля зору більше ніж на 10° у поєднанні з великими абсолютними скотомами — на 10 очах (16,67 %).
За даними оптичної когерентної томографії (ОКТ) макулярної ділянки, перед оперативним лікуванням товщина нейросенсорної сітківки у фовеолярній зоні в середньому становила 315,17 ± 2,31 мкм, товщина судинної оболонки — 264,40 ± 2,89 мкм. При досліджені цілісності пігментного епітелію та хоріокапілярного комплексу встановлено, що на 45 очах (75,0 %) було зниження його оптичної щільності, підвищення оптичної щільності на 5 очах (8,33 %), на 10 очах (16,67 %) змін не зафіксовано. Шар IS/OS був збереженим на 18 очах (30,0 %), на 42 очах (70,0 %) відмічалася його дезорганізація. При проведенні ОКТ диска зорового нерва (ДЗН) у пацієнтів на доопераційному етапі показник RNFL у середньому становив 90,30 ± 1,94 мкм.
При огляді пацієнтів через 1 місяць після оперативного втручання некоригована гострота зору в середньому становила 0,32 ± 0,06. Максимально коригована гострота зору в середньому становила 0,49 ± 0,05. Рівень внутрішньоочного тиску в середньому був 16,9 ± 4,1 мм рт.ст. Офтальмогіпертензія була зафіксована на 2 очах (3,33 %), цим пацієнтам була призначена додатково гіпотензивна терапія у вигляді інстиляцій.
Середній показник світлочутливості сітківки, за даними статичної периметрії Humphrey, становив –4,0 ± 0,5 dB. Показник суми локальних дефектів полів зору становив 3,1 ± 0,1. При дослідженні поля зору за скринінговими тестами нормальні межі поля зору були на 33 очах (55,0 %), мінімальні зміни в полі зору у вигляді відносних парацентральних скотом були на 16 очах (26,67 %), звуження меж поля зору на 5–10° у поєднанні з відносними скотомами — на 8 очах (13,33 %), звуження меж поля зору більше ніж на 10° у поєднанні з абсолютними скотомами — на 3 очах (5,0 %).
За даними ОКТ, товщина нейросенсорної сітківки у фовеолярній зоні в середньому становила 262,34 ± 2,44 мкм, товщина судинної оболонки — 269,40 ± 2,71 мкм. При дослідженні цілісності пігментного епітелію та хоріокапілярного комплексу встановлено, що на 40 очах (66,67 %) було зниження його оптичної щільності, підвищення оптичної щільності на 10 очах (16,67 %), на 10 очах (16,67 %) змін не зафіксовано. Шар IS/OS був збереженим на 47 очах (78,33 %), на 13 очах (21,67 %) відмічалася його дезорганізація. При проведенні ОКТ ДЗН показник RNFL у середньому становив 91,40 ± 1,72 мкм.
При огляді пацієнтів через 3 місяці після оперативного втручання некоригована гострота зору в середньому становила 0,35 ± 0,05. Максимально коригована гострота зору в середньому становила 0,51 ± 0,05. Рівень внутрішньоочного тиску в середньому був 17,2 ± 4,1 мм рт.ст.
Середній показник світлочутливості сітківки, за даними статичної периметрії Humphrey, становив –3,3 ± 0,4 dB. Показник суми локальних дефектів полів зору становив 2,40 ± 0,06. При дослідженні поля зору за скринінговими тестами нормальні межі поля зору були на 35 очах (58,33 %), мінімальні зміни в межах поля зору у вигляді відносних парацентральних скотом були на 17 очах (28,33 %), звуження меж поля зору на 5–10° у поєднанні з відносними скотомами — на 8 очах (13,33 %).
За даними ОКТ, товщина нейросенсорної сітківки у фовеолярній зоні в середньому становила 284,18 ± 2,32 мкм, товщина судинної оболонки — 271,40 ± 2,68 мкм. При дослідженні цілісності пігментного епітелію та хоріокапілярного комплексу встановлено, що на 40 очах (66,67 %) було зниження його оптичної щільності, підвищення оптичної щільності на 10 очах (16,67 %), на 10 очах (16,67 %) змін не зафіксовано. Шар IS/OS був збереженим на 47 очах (78,33 %), на 13 очах (21,67 %) відмічалася його дезорганізація. При проведенні ОКТ ДЗН показник RNFL у середньому становив 90,20 ± 1,85 мкм.
При огляді пацієнтів через 6 місяців після оперативного втручання некоригована гострота зору в середньому становила 0,41 ± 0,05. Максимально коригована гострота зору в середньому становила 0,62 ± 0,05. Рівень внутрішньоочного тиску в середньому був 17,4 ± 3,9 мм рт.ст.
Середній показник світлочутливості сітківки, за даними статичної периметрії Humphrey, становив –2,4 ± 0,5 dB. Показник суми локальних дефектів полів зору становив 2,00 ± 0,08. При дослідженні поля зору за скринінговими тестами нормальні межі поля зору були на 43 очах (71,67 %), мінімальні зміни в межах поля зору у вигляді відносних парацентральних скотом були на 10 очах (16,67 %), звуження меж поля зору на 5–10° у поєднанні з відносними скотомами — на 4 очах (6,67 %), звуження меж поля зору більше ніж на 10° у поєднанні з абсолютними скотомами — на 3 очах (5,0 %).
За даними ОКТ, товщина нейросенсорної сітківки у фовеолярній зоні в середньому становила 278,40 ± 2,78 мкм, товщина судинної оболонки — 265,40 ± 2,85 мкм. При дослідженні цілісності пігментного епітелію та хоріокапілярного комплексу встановлено, що на 40 очах (66,67 %) було зниження його оптичної щільності, підвищення оптичної щільності на 10 очах (16,67 %), на 10 очах (16,67 %) змін не зафіксовано. Шар IS/OS був збережений або відновлений на 52 очах (86,67 %), на 8 очах (13,33 %) зберігалась його дезорганізація. При проведенні ОКТ ДЗН показник RNFL у середньому становив 88,50 ± 1,49 мкм.
Через 1 рік після оперативного втручання було оглянуто 58 пацієнтів (58 очей). Некоригована гострота зору в середньому становила 0,45 ± 0,06. Максимально коригована гострота зору в середньому становила 0,71 ± 0,05. Рівень внутрішньоочного тиску в середньому був 17,6 ± 2,1 мм рт.ст.
Середній показник світлочутливості сітківки, за даними статичної периметрії Humphrey, становив –0,60 ± 0,45 dB. Показник суми локальних дефектів полів зору (PSD) становив 1,30 ± 0,03. При дослідженні поля зору за скринінговими тестами нормальні межі поля зору були на 46 очах (79,31 %), мінімальні зміни в межах поля зору у вигляді відносних парацентральних скотом були на 10 очах (17,24 %), звуження меж поля зору на 5–10° у поєднанні з відносними скотомами — на 2 очах (3,45 %).
За даними ОКТ, товщина нейросенсорної сітківки у фовеолярній зоні в середньому становила 260,30 ± 2,47 мкм, товщина судинної оболонки — 225,60 ± 2,15 мкм. При дослідженні цілісності пігментного епітелію та хоріокапілярного комплексу встановлено, що на 30 очах (51,72 %) було зниження його оптичної щільності, підвищення оптичної щільності на 7 очах (12,01 %), на 21 оці (36,21 %) змін не зафіксовано. Шар IS/OS був збережений або відновлений на 53 очах (91,38 %), на 5 очах (8,62 %) зберігалась його дезорганізація. При проведенні ОКТ ДЗН показник RNFL у середньому становив 87,80 ± 1,36 мкм.
В табл. 1 наведена динаміка гостроти зору в найближчі та віддалені терміни спостереження після ЗСВ з тампонадою вітреальної порожнини газоповітряною сумішшю C3F8, ендолазеркоагуляцією сітківки та ФЕК з імплантацією ІОЛ (M ± m).
Як видно із табл. 1, виконання ЗСВ з тампонадою вітреальної порожнини газоповітряною сумішшю C3F8, ендолазеркоагуляцією сітківки та ФЕК з імплантацією ІОЛ у пацієнтів із регматогенним відшаруванням сітківки у поєднанні з віковою катарактою дозволило статистично значуще підвищити некориговану гостроту зору в 1,8 раза через 1 місяць (t1міс. = 2,8; p < 0,01), у 1,9 раза через 3 місяці (t3міс. = 3,4; p < 0,01), у 2,3 раза через 6 місяців (t6міс. = 4,6; p < 0,01) та у 2,3 раза через 1 рік (t1рік = 4,9; p < 0,01) після оперативного втручання.
Також відмічалося статистично значуще підвищення максимально коригованої гостроти зору в 1,6 раза через 1 та 3 місяці (t1міс. = 3,0, t3міс. = 3,3; p < 0,01), у 2 рази через 6 місяців (t6міс. = 5,2; p < 0,01) та у 2,5 раза через 1 рік (t1рік = 6,8; p < 0,01) після оперативного втручання.
Статистично значуще зниження некоригованої гостроти зору в 3,6 раза на першу добу (t1доба = 6,5, p < 0,01) та в 6,2 раза на десяту добу (t10доба = 6,5, p < 0,01) пов’язане з наявністю у вітреальній порожнині газоповітряної суміші.
В табл. 2 наведена динаміка показників статичної периметрії Humphrey в найближчі та віддалені терміни спостереження після ЗСВ з тампонадою вітреальної порожнини газоповітряною сумішшю C3F8, ендолазеркоагуляцією сітківки та ФЕК з імплантацією ІОЛ (M ± m).
Як видно із табл. 2, виконання ЗСВ з тампонадою вітреальної порожнини газоповітряною сумішшю C3F8, ендолазеркоагуляцією сітківки та ФЕК з імплантацією ІОЛ у пацієнтів із регматогенним відшаруванням сітківки у поєднанні з віковою катарактою дозволило статистично значуще підвищити світлочутливість сітківки (MD) в 1,5 раза через 1 місяць (t1міс. = 3,2; p < 0,01), у 1,9 раза через 3 місяці (t3міс. = 4,2; p < 0,01), у 2,6 раза через 6 місяців (t6міс. = 5,6; p < 0,01) та у 10,2 раза через 1 рік (t1рік = 9,2; p < 0,01) після оперативного втручання, а також статистично значуще знизити локальні дефекти полів зору (PSD) в 1,4 раза через 1 місяць (t1міс. = 6,8; p < 0,01), у 1,8 раза через 3 місяці (t3міс. = 14,6; p < 0,01), у 2,2 раза через 6 місяців (t6міс. = 17,5; p < 0,01) та у 3,3 раза (t1рік = 24,5; p < 0,01) через 1 рік після оперативного втручання.
/36.jpg)
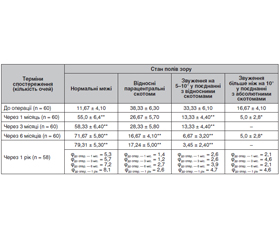
В табл. 3 наведена динаміка показників поля зору за скринінговими тестами в найближчі та віддалені терміни спостереження після ЗСВ з тампонадою вітреальної порожнини газоповітряною сумішшю C3F8, ендолазеркоагуляцією сітківки та ФЕК з імплантацією ІОЛ (M ± m).
Як видно із табл. 3, виконання ЗСВ з тампонадою вітреальної порожнини газоповітряною сумішшю C3F8, ендолазеркоагуляцією сітківки та ФЕК з імплантацією ІОЛ у пацієнтів із регматогенним відшаруванням сітківки у поєднанні з віковою катарактою дозволило статистично значуще нормалізувати межі поля зору в 4,7 раза через 1 місяць спостережень (φ1міс. = 5,3; p < 0,01), у 5 разів через 3 місяці (φ3міс. = 5,7; p < 0,01), у 6,1 раза через 6 місяців (φ6міс. = 7,2; p < 0,01) та у 6,8 раза через 1 рік (φ1рік = 8,1; p < 0,01) після оперативного втручання, а також знизити зміни у полі зору у вигляді відносних парацентральних скотом в 2,3 раза через 6 місяців (φ6міс. = 2,7; p < 0,01) та 2,2 раза (φ1рік = 2,6; p < 0,01); звуження на 5–10° у поєднанні з відносними скотомами в 2,5 раза через 1 та 3 місяці спостережнь (φ1, 3міс. = 2,6; p < 0,01), у 5 разів через 6 місяців (φ6міс. = 3,9; p < 0,01) та 9,7 раза через 1 рік (φ1рік = 4,7; p < 0,01); звуження поля зору більше ніж на 10° у поєднанні з абсолютними скотомами в 3,3 раза через 1 та 6 місяців спостережень (φ1, 6міс. = 2,1; p < 0,05) порівняно з даними до оперативного втручання.
В табл. 4 наведена динаміка товщини нейросенсорної сітківки у фовеолярній зоні в найближчі та віддалені терміни спостереження після ЗСВ з тампонадою вітреальної порожнини газоповітряною сумішшю C3F8, ендолазеркоагуляцією сітківки та ФЕК з імплантацією ІОЛ (M ± m).
Як видно із табл. 4, після виконання ЗСВ з тампонадою вітреальної порожнини газоповітряною сумішшю C3F8, ендолазеркоагуляцією сітківки та ФЕК з імплантацією ІОЛ у пацієнтів із регматогенним відшаруванням сітківки у поєднанні з віковою катарактою статистично значуще зменшується товщина нейросенсорної сітківки у фовеолярній зоні через 1 місяць спостережнь на 23 % (t1міс. = 6,9, p < 0,01), на 33 % через 3 місяці (t3міс. = 9,9; p < 0,01), на 30 % через 6 місяців (t6міс. = 9,6; p < 0,01) та на 22 % через 1 рік (t1рік = 6,5; p < 0,01) після оперативного втручання.
В табл. 5 наведена динаміка товщини судинної оболонки в найближчі та віддалені терміни спостереження після ЗСВ з тампонадою вітреальної порожнини газоповітряною сумішшю C3F8, ендолазеркоагуляцією сітківки та ФЕК з імплантацією ІОЛ (M ± m).
Як видно із табл. 5, після виконання ЗСВ з тампонадою вітреальної порожнини газоповітряною сумішшю C3F8, ендолазеркоагуляцією сітківки та ФЕК з імплантацією ІОЛ у пацієнтів із регматогенним відшаруванням сітківки у поєднанні з віковою катарактою спостерігалося статистично значуще зниження товщини судинної оболонки на 17 % через 1 рік спостережень (t1рік = 4,9; p < 0,01) після оперативного втручання.
В табл. 6 наведена динаміка стану пігментного епітелію та хоріокапілярного комплексу в найближчі та віддалені терміни спостереження після ЗСВ з тампонадою вітреальної порожнини газоповітряною сумішшю C3F8, ендолазеркоагуляцією сітківки та ФЕК з імплантацією ІОЛ (у відсотках, Р ± m).
Як видно із табл. 6, після виконання ЗСВ з тампонадою вітреальної порожнини газоповітряною сумішшю C3F8, ендолазеркоагуляцією сітківки та ФЕК з імплантацією ІОЛ у пацієнтів із регматогенним відшаруванням сітківки у поєднанні з віковою катарактою через 1 рік статистично значуще в 2,2 раза (φ1рік = 2,4; p < 0,01) підвищилася кількість очей, які не мали змін пігментного епітелію та хоріокапілярного комплексу, зменшилася в 1,5 раза (φ1рік = 2,7; p < 0,01) кількість очей зі зниженням оптичної щільності пігментного епітелію та хоріокапілярного комплексу.
В табл. 7 наведена динаміка стану шару IS/OS в найближчі та віддалені терміни спостереження після ЗСВ з тампонадою вітреальної порожнини газоповітряною сумішшю C3F8, ендолазеркоагуляцією сітківки та ФЕК з імплантацією ІОЛ (у відсотках, Р ± m).
Як видно із табл. 7, після виконання ЗСВ з тампонадою вітреальної порожнини газоповітряною сумішшю C3F8, ендолазеркоагуляцією сітківки та ФЕК з імплантацією ІОЛ у пацієнтів із регматогенним відшаруванням сітківки у поєднанні з віковою катарактою через 1 та 3 місяці статистично значуще в 2,6 раза (φ1, 3міс. = 5,6; p < 0,01), через 6 місяців у 2,9 раза (φ6міс. = 6,8; p < 0,01), через 1 рік у 3 рази (φ1рік = 7,5; p < 0,01) підвищилася кількість очей із збереженим або відновленим шаром IS/OS після оперативного втручання порівняно з даними до оперативного втручання.
У табл. 8 наведена динаміка показника RNFL у найближчі та віддалені терміни спостереження після ЗСВ з тампонадою вітреальної порожнини газоповітряною сумішшю C3F8, ендолазеркоагуляцією сітківки та ФЕК з імплантацією ІОЛ (M ± m).
Як видно із табл. 8, після виконання ЗСВ з тампонадою вітреальної порожнини газоповітряною суміш–шю C3F8, ендолазеркоагуляцією сітківки та ФЕК з імплантацією ІОЛ у пацієнтів із регматогенним відшаруванням сітківки у поєднанні з віковою катарактою відмічається зниження показника RNFL через 6 місяців та 1 рік спостережень, але ці дані були статистично незначущі.
Обговорення
Комбінована операція — закрита субтотальна вітректомія і факоемульсифікація катаракти є ефективною і безпечною процедурою, яка забезпечує якісне видалення задньої і передньої гіалоїдної мембрани та безпечні маніпуляції хірурга у вітреальній порожнині без ушкодження кришталика. Така стратегія призводить до мінімізації хірургічної травми, знижує ризик ускладнень і сприяє швидкому відновленню зору. Як тампонуючу речовину під час ЗСВ ми використовували перфторпропан (C3F8), який збільшувався в об’ємі в 4 рази і мав час розсмоктування приблизно 55–65 днів. Інші гази мають менший об’єм та менший час розсмоктування. Наприклад, сульфургексафторид (SF6) збільшується в об’ємі в 2 рази, час розсмоктування газової бульбашки 10–14 днів, перфторетан (C2F6) збільшується в об’ємі в 3 рази, час розсмоктування 30–35 днів. Ефективність тампонади C3F8 завдяки збільшенню об’єму та більш тривалому розсмоктуванню сприяє високому анатомічному та функціональному результату [14].
Отже, проведені нами дослідження упродовж 1 року встановили, що виконання ЗСВ з тампонадою вітреальної порожнини газоповітряною сумішшю C3F8, ендолазеркоагуляцією сітківки та ФЕК з імплантацією ІОЛ є ефективним методом оперативного лікування пацієнтів із регматогенним відшаруванням сітківки у поєднанні з віковою катарактою, який дозволяє отримати задовільні анатомічні та функціональні результати.
Висновки
1. Виконання ЗСВ з тампонадою вітреальної порожнини газоповітряною сумішшю C3F8, ендолазеркоагуляцією сітківки та факоемульсифікацією з імплантацією ІОЛ у хворих із регматогенним відшаруванням сітківки у поєднанні з віковою катарактою дозволило через 1 рік спостережень статистично значуще підвищити: некориговану та максимально кориговану гостроту зору.
2. Після виконання комбінованого хірургічного втручання відмічається статистично значуща нормалізація показників статичної периметрії та показників скринінгових тестів через 1 рік спостережень.
3. Застосування ЗСВ з тампонадою вітреальної порожнини газоповітряною сумішшю C3F8, ендолазеркоагуляцією сітківки та факоемульсифікацією з імплантацією ІОЛ дозволяє статистично значуще поліпшити морфофункціональні показники сітківки та судинної оболонки у хворих із регматогенним відшаруванням сітківки у поєднанні з віковою катарактою через 1 рік спостережень.
Конфлікт інтересів. Автор заявляє про відсутність конфлікту інтересів та власної фінансової зацікавленості при підготовці даної статті.
Отримано/Received 09.07.2022
Рецензовано/Revised 20.07.2022
Прийнято до друку/Accepted 01.08.2022

/35.jpg)
/36.jpg)
/37.jpg)
/38.jpg)
/39.jpg)