Інсиденталоми надниркових залоз (НЗ) — збірна робоча категорія, що містить широкий діапазон різних форм патології даних залоз. Вони відрізняються за вихідними тканинними структурами, з яких беруть свій початок, клінічними і гормональними характеристиками, діагностичними і тактичними підходами. Настільки широкий спектр захворювань НЗ, які ховаються під маскою випадково виявленої інсиденталоми, висуває перед клініцистом завдання їх ідентифікації (установлення клінічного і, якщо можливо, морфологічного діагнозу) із визначенням тактичних підходів [1, 2].
У світлі цього при встановленні інсиденталоми НЗ клініцист зобов’язаний розв’язати три основні питання, з яких перші два є діагностичними, а третє — тактичним. Сформулювати їх можна так:
— чи є виявлене утворення доброякісним або злоякісним;
— чи є виявлене утворення гормонопродукуючим або гормонально-неактивним;
— чи слід оперувати хворого або обмежитися спостереженням?
Відповідь на перші два питання дозволить із найбільшою вірогідністю встановити клінічний діагноз, після чого буде можливо переходити до вирішення третього.
Приступаючи до розгляду поставлених питань, насамперед необхідно визначити нозологічну приналежність тіні, виявленої на екрані апарата ультразвукової діагностики (УЗД), комп’ютерної томографії (КТ) або магнітно-резонансної томографії (МРТ). Як вказано вище, це можуть бути різні види пухлин і пухлиноподібних утворень, природу яких можна встановити за допомогою аналізу даних клінічних, візуалізуючих і гормонально-біохімічних досліджень.
Результати численних епідеміологічних досліджень дозволяють отримати уявлення про різноманітність виявлених інсиденталом НЗ. Група італійських авторів зібрала відомості про 1004 інсиденталоми НЗ із 26 центрів [3]. За характеристиками візуалізуючих методів і даними гормональних досліджень, 85 % виявлених утворень не мали гормональної активності. Серед решти в 9,2 % випадків був виявлений субклінічний синдром Кушинга, у 4,2 % — феохромоцитома, у 4,68 % — карцинома, у 1,6 % — альдостерома, у 1,2 % — метастази в НЗ. Із загальної кількості хворих були прооперовані 380 осіб. За результатами гістологічного дослідження видалених утворень діагноз аденоми кори НЗ був установлений у 52 % випадків (198 хворих), серед яких 69 % — гормонально-неактивні і 25 % — кортизолпродукуючі аденоми, 6 % — адьдостероми. Феохромоцитоми становили 11 %, рак — 12 %, метастази в НЗ — 2 %, мієлоліпоми — 8 %, кісти — 5 %, гангліоневроми — 4 %, інші — 6 %.
Японські дослідники [4] повідомили про 2455 інсиденталом, у числі яких 52,3 % — нефункціонуючі доброякісні аденоми, 7,9 % — кортизолпродукуючі пухлини, 7,9 % — феохромоцитоми, 4,1 % — альдостероми, 1,5 % — карциноми. Дещо іншим виявився аналіз характеристик 1049 інсиденталом, наведений їх співвітчизниками [5], у хворих, відібраних з урахуванням відсутності злоякісних захворювань й ознак адреналової гіперфункції. Серед них доброякісні аденоми становили 75 %, мієлоліпоми — 6 %, гематоми — 4 %, кісти — 1 %, феохромоцитоми — 0,3 %.
Зведена статистика [6] 26 авторів, що містить відомості про 3868 інсиденталом НЗ, була представлена такими нозологічними одиницями: функціонуючі аденоми — 71,2 % (36,7–96,1), аденоми із субклінічним синдромом Кушинга — 7,9 % (1,0–47,4), феохромоцитоми — 5,6 % (0–23,3), альдостероми — 1,2 % (0–4,8). Первинні карциноми в середньому становили 6,2 % (0–9,4), причому в 10 серіях даний показник дорівнював 0, у 8 — 1–10 % і в 6 — понад 10 %. Частка метастазів у НЗ становила 2,1 % (0–11,1), інші пухлини — 7,6 %. Сумарно доброякісним захворюванням відповідали 85,9 % інсиденталом.
Одним із найбільших відомих оглядів, присвячених інсиденталомам НЗ, є робота G. Mansmann et al. [7]. У ній автори провели аналіз світової літератури із цієї проблеми за 1966–2001 рр. Із понад 5000 робіт, які стосуються зазначеної теми, було відібрано 699 основних публікацій, що лягли в основу характеристики проблеми. Цифрові викладки базувалися на розгляді матеріалів 44 базових публікацій (серій); для додаткового підтвердження окремих положень використовувалися роботи, які не увійшли до цього переліку. Більшість виявлених інсиденталом НЗ були доброякісними аденомами, які траплялися з частотою 36–94 % (у середньому — 60 %) серед всіх інсиденталом. 65 % аденом були розміром менше 6,0 см, і 18 % — більше. Серед них певна частина була гормоносекретуючими. Так, гіперсекреція кортизолу виявлялася в 5–47 % випадків, альдостерону — у 1,6–3,3 %. Феохромоцитоми становили в середньому 8 % (5–47). Первинний рак кори НЗ виявлявся в 10,0 % випадків, і метастази в НЗ пухлин інших локалізацій — у 19,0 %. Підтверджено збільшення ризику малігнізації залежно від розмірів інсиденталоми, про що сказано вище і в осіб з онкологічним анамнезом, у яких 50–75 % інсиденталом є метастазами. До 20–25 % діагностованих інсиденталом виявляються мієлоліпомою, ліпомою, ліпосаркомою, гангліоневробластомою, гамартомою, лімфомою. Певну частку становлять кісти, гематоми, запальні пухлини (абсцес, туберкулома).
Виконані порівняльні дослідження [8] нозологічної структури інсиденталом НЗ ґрунтуються на даних клінічного обстеження (перша група) і постхірургічних результатах (друга група). При цьому частота аденом істотно відрізняється за клінічними даними й операційними знахідками — 80 % (33–96) і 55 % (40–69) відповідно. Це можна пояснити тим, що значна кількість виявлених інсиденталом не перевищує розмірів 1,0–2,0 см і не потребує оперативного втручання за відсутності в них ознак злоякісності. Частота функціонально неактивних інсиденталом істотно не відрізнялася і дорівнювала 75 % (71–84) і 69 % (52–75) відповідно в обох групах. Також не спостерігалося вірогідних відмінностей у частоті кортизолпродукуючих аденом — 12 % (1–29) і 10 % (1–15). Щоправда, альдостеронпродукуючі аденоми частіше спостерігалися в другій групі — 6 % (2–7) порівняно з першою — 2,5 % (1,6–3,3). Майже однаково часто спостерігалася феохромоцитома: 7 % (1,5–14) і 10 % (11–23). Карцинома НЗ дещо частіше відзначалася у хворих другої групи — 11 % (1,2–12), ніж у першій — 8 % (1,2–11). Можливо, це пов’язано з тим, що в частини хворих діагноз установлювали на підставі остаточного гістологічного дослідження. Метастатичні пухлини виявлялися майже однаково часто: 5 % (0–18) і 7 % (0–21). У числі оперованих інсиденталом спостерігалися кісти (5 %), мієлоліпоми (8 %), гангліоневроми (4 %). Наведені дані свідчать, що здебільшого можливі правильна ідентифікація і визначення показань для хірургічного лікування інсиденталом НЗ.
Корейські автори [9] з огляду на дані лікування 348 хворих повідомляли про 6,2 % випадків (2,1–20) феохромоцитом, 8,1 % (3–11,3) — субклінічного синдрому Кушинга, 3,9 % (1,5–10) — альдостером, 2,6 % (0,7–15) — первинного та метастатичного раку НЗ. W. Young Jr. [10] на підставі аналізу 13 публікацій, що містять відомості про 2005 виявлених інсиденталом НЗ, наводить такі дані. Частка аденом із субклінічним синдромом Кушинга становила в середньому 5,3 %, феохромоцитом — 5 %, альдостером — 1 %. Первинна карцинома була виявлена в 4,7 % випадків, і метастази в НЗ — в 2,5 %.
Певний інтерес становить розподіл основних варіантів інсиденталом НЗ — аденоми, феохромоцитоми, карциноми за географічною ознакою. Із цією метою були розглянуті дані 18 робіт з Європи (2586 інсиденталом), 11 — із США (1171 випадок) і 7 (547) — з Азії. У європейських серіях частота аденом у середньому становила 52,6 % (18–82). За даними американських досліджень, дані показники дорівнювали 67,6 % (21–97), й азіатських — 41 % (12–85). У європейських роботах частота феохромоцитоми серед інсиденталoм дорівнювала 5,05 % (0–17), в американських — 3,7 % (0–11) й азіатських — 12,6 % (0–23). Первинний рак НЗ у серії європейських робіт спостерігався в середньому з частотою 5,6 % (0–13). У роботах зі США дані показники дорівнювали 3,7 % (0–6), і з Азії — 12,65 % (0–23). Сумарно спостерігається майже однакова частота аденом серед інсиденталом у Європі й Америці і трохи нижче — в Азії. При невеликих відмінностях частоти феохромоцитоми у Європі й Америці в Азії вона вище у 2,5 раза, ніж у Європі, і в 3,4 раза — ніж в Америці. Відзначається також перевищення частоти первинного раку серед інсиденталом в Азії порівняно з Європою у 2,2 раза й Америкою — у 3,4 раза [11–13].
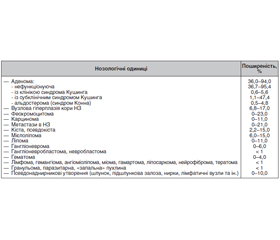
На підставі аналізу наведених даних, а також численних публікацій, що не увійшли в даний огляд, можливо орієнтовно сумарно уявити нозологічну структуру і поширеність окремих форм у категорії «інсиденталоми НЗ» (табл. 1), а також запропонувати їх робочу класифікацію. Значний розкид даних, наведених у таблиці, можна зрозуміти. В окремих серіях хворих вони були отримані при використанні різних методик дослідження (УЗД, КТ, часткове або повне гормональне обстеження). Контингенти обстежених були дуже варіабельні: групи здорових осіб, відібраних для скринінгових обстежень, хворі з патологією органів черевної порожнини, артеріальною гіпертензією, цукровим діабетом, різні вікові групи й ін. Деякі серії налічували невелику кількість спостережень, і встановлення поширеності інсиденталом у них давало високі процентні показники.
Нижче наводиться класифікація інсиденталом НЗ за морфогенезом і функціональною активністю.
1. Інсиденталома з кори НЗ — аденома, карцинома, вузлова гіперплазія:
а) гормоносекретуча: кортизол (субклінічний/маніфестний синдром Кушинга), альдостерон (синдром Конна), андрогени/естрогени (синдром вірилізації/фемінізації);
б) гормонально-неактивна.
2. Інсиденталома з мозкової речовини НЗ — феохромоцитома: доброякісна/злоякісна, секретуюча катехоламіни/гормонально-неактивна.
3. Інсиденталома з жирової, гемопоетичної, сполучної, лімфоїдної тканини, судин: доброякісна/злоякісна, що не має гормональної активності: мієлоліпома, ліпома, нейрофіброма, гамартома, тератома, лімфома, лейоміома, лейоміосаркома, гангліоневрома, невробластома.
4. Інсиденталома — пухлиноподібне утворення: кіста, гранульома, ехінококоз, ксантоматоз, амілоїдоз, гранульома, абсцес, гематома.
5. Інсиденталома — метастаз у НЗ злоякісної пухлини іншої локалізації (молочна залоза, легені, печінка, нирка, кишечник, передміхурова залоза).
6. Інсиденталома — псевдонаднирникове утворення, що походить із печінки, підшлункової залози, нирки, селезінки, кишечника, лімфатичних вузлів.
7. Технічні артефакти в результаті появи додаткових тіней під час дослідження.
Маючи уявлення про те, які форми патології (захворювання) НЗ приховуються під маскою інсиденталоми, приступають до вирішення таких питань. З якою саме конкретної пухлиною або пухлиноподібним утворенням стикається клініцист: чи є воно гормоносекретуючим або гормонально-неактивним і чи є воно доброякісним або злоякісним. Існують доволі численні настанови і ще більша кількість оглядових статей з авторитетних клінік, які регламентують порядок обстеження хворих із виявленою інсиденталомою НЗ. Вони містять рекомендації з використання різних діагностичних методик (клінічні, гормональні, візуалізуючі) і пропонують трактування отриманих даних. Зібрана інформація зазвичай є основою створення алгоритмів діагностики. Установлення остаточного або майже остаточного діагнозу слугує базою для прийняття рішення щодо тактичних підходів до виявленої патології: оперативне лікування, консервативна терапія, спостереження [14–17].
Виявлення інсиденталоми НЗ передбачає одночасне паралельне обстеження хворого, що містить комплекс горональних і біохімічних досліджень, а також оцінку даних візуалізуючої діагностики. За потреби остання повторюється або використовується інший метод. Одночасно необхідне ретельне клінічне обстеження хворого. Доцільно з’ясувати наявність характерних специфічних і неспецифічних симптомів і синдромів, що супроводжують різні форми гіпер- і гіпокортицизму, феохромоцитоми, гормонально-неактивних пухлин, злоякісних і доброякісних. До них можна віднести такі, як зміна зовнішнього вигляду, збільшення маси тіла, схуднення, переломи кісток, слабкість, біль, порушення функцій кишечника, дизуричні явища тощо. Особливе значення мають наявність артеріальної гіпертензії та оцінка характеру її перебігу (постійна, пароксизмальна, стійка до антигіпертензивної терапії та ін.), серцево-судинного захворювання, цукрового діабету, остеопорозу, порушень жирового, вуглеводного, мінерального обміну [18].
Трактування даних топічної діагностики дозволяє максимально наблизитися до розв’язання питання: виявлене утворення доброякісне або злоякісне? Методом вибору способу візуалізації НЗ та їх пухлин є оглядова КТ, за потреби — із контрастним підсиленням. Якщо пухлина раніше була виявлена за допомогою УЗД, необхідно провести КТ, оскільки з її допомогою можна отримати більш конкретні й об’єктивні характеристики досліджуваного об’єкта. При її сумнівних результатах слід скористатися МРТ або позитронно-емісійною томографією в поєднанні з КТ. КТ має високу роздільну здатність, що дає можливість визначити тканинну щільність утворення і низку показників, які дозволяють судити про його доброякісний або злоякісний характер. Щільність пухлини виражається в одиницях Хаунсфілда (Hu). Для доброякісних, багатих ліпідами аденом НЗ даний показник щільності дорівнює менше 10 од. Hu. Однак близько 30 % доброякісних аденом НЗ бувають бідними на ліпіди, та їх щільність перевищує 10 од. Hu. Дана ознака також спостерігаються при злоякісних пухлинах кори НЗ і феохромоцитомі. У подібних випадках слід вдатися до контрастної КТ із підсиленням [19].
Доброякісні аденоми мають здатність швидко накопичувати і виводити введену контрастну речовину порівняно зі злоякісними, при яких ці процеси бувають уповільненими. Установлено, що для доброякісних пухлин характерні високі відносні — більше 40 % й абсолютні величини вимивання контрастної речовини — понад 60 %. При злоякісних пухлинах дані показники вірогідно нижчі [20].
Крім оцінки щільності інсиденталом, використовуються ще деякі показники оглядової і контрастної КТ для диференціації злоякісних і доброякісних новоутворень. Насамперед це розміри пухлини. Вище вказувалося, що в міру збільшення розмірів пухлини ризик її злоякісності зростає. Якщо при пухлинах до 4,0 см він становить 2 %, то при величинах 4,1–6,0 см він збільшується утричі і більше 6,0 см — у 12,5 раза. У сучасній клінічній практиці розмір пухлини більше 4,0 см є одним з основних, якщо не головним, при визначенні показань для оперативного лікування інсиденталоми. Деякі хірурги виділяють групу пухлин розмірами в 4,1–6,0 см, які відносять до розряду «сірої шкали», в межах якої питання про операцію вирішується індивідуально з урахуванням низки факторів. Пухлини розміром понад 6,0 см однозначно підлягають оперативному лікуванню, якщо дозволяє стан хворого.
Для доброякісних інсиденталом — аденом характерні рівномірна щільність (< 10 од. Hu), правильна округла форма, чіткі контури, диференційована капсула, відсутність ознак інвазії в навколишні структури. Злоякісні пухлини мають підвищену, часто нерівномірну щільність (> 10 од. Hu). У них можуть бути вогнища некрозу, кальцієві включення. Вони нерідко мають неправильну форму, нечітку капсулу або бувають представлені конгломератом вузлів. Важливе значення мають ознаки інвазії пухлини в навколишні структури.
МРТ є більш ефективним методом візуалізації і диференціації пухлин НЗ. Зазвичай до проведення МРТ рекомендують вдаватися при отриманні непереконливих даних КТ. Іншою перевагою МРТ є відсутність променевого навантаження та необхідності введення контрастної речовини. Як метод вибору вона рекомендується при обстеженні вагітних жінок, дітей, підлітків і навіть у деяких випадках осіб до 30 років [21].
Визначення гормонального статусу виявленої інсиденталоми НЗ дозволяє спільно з даними топічної діагностики оцінити її нозологічну приналежність й остаточно вирішити питання про подальшу тактику. Відповідно до наявності трьох груп кортикостероїдів, які продукуються корою НЗ (глюко-, мінералокортикоїди, статеві гормони), за певними показниками, рекомендується дослідження кортизолу, альдостерону і статевих гормонів [22].
Для виявлення глюкокортикоїдної активності інсиденталоми найбільш об’єктивним і поширеним є нічний супресивний тест із навантаженням 1 мг дексаметазону, чутливість якого досягає 98,1 % і специфічність — 80,5–98,9 %. Нормальним результатом у здорових осіб вважається зниження рівня кортизолу в крові < 5,0 мкг/дл (< 138,0 нмоль/л). Інтервал від 5,0 до 10,0 мкг/дл (50–138 нмоль/л) передбачає можливість наявності автономного субклінічного гіперкортицизму, тоді як цифри понад 10,0 мкг/дл (> 138 нмоль/л) характерні для маніфестного синдрому Кушинга [23]. Існують певні розбіжності щодо даних граничних величин, тому пропонуються як контрольні показники від 1,0 до 5,0 мкг/дл (27,6–138,0 нмоль/л). Наприклад, у багатьох клініках Великобританії вважають, що зниження кортизолу плазми менше 1,8 мкг/дл (50,0 нмоль/л) дозволяє вірогідно виключити автономний гіперкортицизм, хоча в подібній ситуації збільшується частота хибно-позитивних результатів. Проба з 1 мг дексаметазону показана всім хворим із виявленою інсиденталомою НЗ. У разі сумнівних результатів проби рекомендується додатково визначати вміст кортизолу в плазмі, сечі, добовий ритм секреції кортизолу, проводити проби з 2 і 8 мг дексаметазону, визначення кортизолу в нічний слині. Істотна роль належить дослідженню адренокортикотропного гормона у плазмі, особливо в поєднанні з результатами проби з 1,0 мг дексаметазону.
Тут було б доцільно згадати про виявлення, особливо у зв’язку з інсиденталомою НЗ, варіанти автономного глюкокортикоїдного гіперкортицизму, що отримав назву «субклінічний синдром Кушинга». Він був уперше описаний W. Beierwaltes et al. [24]. Дане поняття включало характеристики пухлин НЗ, які автономно продукують невеликі кількості кортизолу, недостатні для розвитку типової картини синдрому Кушинга, але здатні пригнічувати продукцію адренокортикотропного гормона. Результатом буває наявність окремих синдромів Кушинга (артеріальна гіпертензія, цукровий діабет), зниження стимуляції протилежної надниркової залози і ризик розвитку гострого гіпокортицизму в разі видалення надниркової залози, ураженої пухлиною. Деякі дослідники віддають пріоритет в описі субклінічного синдрому Кушинга B. Charbonell et al. [25], які сформулювали дане поняття так: інсиденталома НЗ з автономною нерегульованою продукцією глюкокортикоїдів, але без специфічних ознак і симптомів, притаманних клінічно явному синдрому Кушинга. У подальшому до субклінічного синдрому Кушинга визнали можливим умовно відносити не тільки випадки з відсутністю симптоматики гіперкортицизму, але й хворих із наявністю окремих ознак синдрому або їх поєднань, виявлених у різних ступенях (артеріальна гіпертензія, ожиріння, порушена толерантність до глюкози, дисліпідемія, остеопороз). Їх навіть класифікували як пре-Кушинг, розглядаючи як ранню стадію захворювання або порушення функцій НЗ. Підтвердженням є той факт, що в багатьох хворих вони ліквідовувалися або їх перебіг зм’якшувався після адреналектомії з аденомою.
Як виявилося, субклінічний синдром Кушинга не є великою рідкістю. За сумарними даними 22 дослідників [26], серед 2622 хворих з інсиденталомою НЗ у 236 (9,0 %) випадках був виявлений субклінічний синдром Кушинга при коливаннях даного показника в межах 1,1–47,3 % в окремих серіях. Привертає увагу велика варіабельність частоти виявлення субклінічного синдрому Кушинга, що, можливо, пов’язано з використанням різних критеріїв для віднесення окремих випадків до цієї категорії.
Первинний гіперальдостеронізм (синдром Конна) супроводжує інсиденталому набагато рідше, ніж субклінічний синдром Кушинга. Підозри на користь наявності синдрому Конна у хворих з інсиденталомою виникають за наявності артеріальної гіпертензії, особливо стійкої до антигіпертензивної терапії, гіпокаліємії, м’язової слабкості, порушення ниркових функцій. Частота синдрому Конна серед інших видів інсиденталом не перевищує 2 %, рідко досягає 3–4 %. Останнім часом поширеність альдостером серед хворих з інсиденталомами НЗ зросла до 7–35 % у зв’язку з описом варіантів гіперальдостеронізму з нормокаліємією. Найбільш широко рекомендованим скринінговим тестом для пошуку гіперальдостеронізму, у тому числі й у хворих з інсиденталомою НЗ, є дослідження співвідношення вмісту альдостерону в плазмі до активності реніну. Вважається, що даний показник вище 20 (деякі вважають вище 30) є вагомим аргументом на користь наявності синдрому Конна. При величинах > 50 діагноз стає абсолютним, коли рівень альдостерону виражається в нг/дл й активність реніну — у нг/мл/год. Чутливість тесту становить до 90 %, специфічність — до 91 %. При показниках в інтервалі 20/30–50 для підтвердження діагнозу рекомендується проведення функціональних проб [27].
Останнім часом у багатьох настановах рекомендується проводити дані дослідження тільки за наявності артеріальної гіпертензії у хворого з інсиденталомою НЗ. Із цим складно погодитися. У деяких хворих артеріальний тиск може незначно або періодично підвищуватися без характерних симптомів або він не вимірюється тривалий час і демонстративні ознаки бувають не виражені. У таких хворих можуть бути граничні рівні співвідношення альдостерон/ренін, знижений рівень калію, періодичні незареєстровані епізоди підвищення артеріального тиску, м’язової слабкості, головного болю, ниркові порушення, що буває характерним для гіперальдостеронізму, особливо його початкових або субклінічних форм. Ці доводи повинні свідчити на користь доцільності дослідження мінералокортикоїдної функції кори НЗ у хворих з інсиденталомою, можливо, за індивідуальними показаннями [28].
Інсиденталоми з клінікою гіперсекреції статевих гормонів — андрогенів або естрогенів трапляються вкрай рідко. Це можуть бути аденоми або первинні карциноми кори НЗ. У деяких настановах вказується, що у хворих з інсиденталомою НЗ за відсутності клінічних ознак вірилізації в жінок і фемінізації в чоловіків дослідження статевих стероїдів не показане. Слід підкреслити, що для правильного розв’язання цього питання виняткове значення мають результати клінічного обстеження, де слід враховувати найменші симптоми ефекту надлишку статевих гормонів. Так, наявність навіть помірного гірсутизму в поєднанні з розладами менструального циклу в жінок може свідчити на користь андростероми, а гінекомастія, зниження потенції у чоловіків — на користь кортикоестроми. Ці і деякі інші симптоми повинні слугувати відправними ознаками для дослідження андрогенів у першому випадку й естрогенів — у другому. Зазвичай рекомендується дослідження тестостерону і його метаболітів при підозрі на андростерому в жінок і естрогенів, сумарних та фракційних, при підозрі на кортикоестрому — у чоловіків. Окремо слід згадати значення дослідження дегідроепіандростерону-C, збільшення вмісту якого розцінюється багатьма фахівцями як ознака надлишкової продукції андрогенів і маркер злоякісності. Відзначено, що чутливість даного показника при диференціації доброякісних аденом і карцином НЗ досягає 100 % і специфічність — 47 %. Рішення про необхідність дослідження статевих гормонів приймається індивідуально [29].
Ідентифікація інсиденталоми НЗ як феохромоцитоми повинна здійснюватися насамперед з огляду на небезпеку для хворого супутніх даним пухлинам розладів кровообігу, часто — із несприятливими наслідками. Крім основних форм хромафінних пухлин із клінікою пароксизмальної, змішаної і постійної артеріальної гіпертензії, часто відмічаються клінічно німі новоутворення, які дають про себе знати лише при певних ситуаціях (стрес, фізичні навантаження, операція, наркоз) у вигляді тяжких кризів артеріальної гіпертензії із серйозними розладами кровообігу. До 50 % випадків феохромоцитом, які виявляються як інсиденталоми, супроводжуються нормотензією. Пацієнти з випадково виявленою феохромоцитомою зазвичай більш старшого віку, ніж хворі із симптомними пухлинами, і в них зазвичай відсутні клінічні симптоми й ознаки, що дозволяють думати про феохромоцитому. Тому всім хворим з інсиденталомою НЗ однозначно показане гормональне і біохімічне обстеження на предмет виключення або підтвердження наявності феохромоцитоми [30].
Методом вибору гормональної діагностики феохромоцитоми залишається дослідження вмісту катехоламінів — адреналіну і норадреналіну в плазмі або сечі і/або їх метаболітів. Концентрація сумарних катехоламінів у плазмі нижче 500,0 пг/мл дозволяє виключити феохромоцитому, рівень понад 2000,0 пг/мл вірогідно підтверджує діагноз. В останні декілька десятиліть найкращим методом діагностики вважають визначення в плазмі метанефринів, метильованих метаболітів адреналіну і норадреналіну: метанефрину, норметанефрину, ванілілмигдальної кислоти. Роздільне дослідження даних сполук більшістю дослідників визнається тестами першої лінії як для діагностики феохромоцитоми, так і для виявлення інсиденталоми НЗ. Дослідження слід виконувати не менше двох разів. При проміжних величинах показників рівнів катехоламінів і метаболітів рекомендується проведення функціональних проб, провокаційних і/або адренолітичних. З огляду на те, що до 25 % хромафінних пухлин мають спадковий, генетично обумовлений характер, при виявленні серед інсиденталом феохромоцитоми таким хворим показано додаткове обстеження на предмет виявлення в них синдрому МЕН-2, хвороби Гіппеля — Ліндау, Реклінгаузена I типу, синдромів Лі — Фраумені, Карнея, Беквіта — Відемана, сімейного аденоматозного поліпозу [31].
Частка первинного адренокортикального раку серед інсиденталом НЗ виявляється досить реальною, незважаючи на рідкість його в загальній популяції. Випадково виявлені карциноми НЗ у 26–94 % випадків є гормонопродукуючими. Настільки широкий діапазон пояснюється тим, що деякі дослідники включають у групу гормонально активних не тільки пухлини з клінікою синдромів (Кушинга, вірилізації й ін.), але й випадки, що супроводжуються збільшенням рівнів певних гормонів без клінічних проявів. Спостерігається лінійна залежність частоти виявлення карцином від розмірів інсиденталоми, що відзначалося вище. Злоякісні інсиденталоми частіше визначаються, коли вони досягають значних розмірів і можуть супроводжуватися локальним масефектом і віддаленими метастазами [32].
Злоякісний характер інсиденталом визначається за наявністю ознак, описаних више. Усе ще залишається дискутабельним питання: чи є інсиденталоми метастазами утворень, які виявляються в осіб з онкологічним анамнезом Крім того, більшість клініцистів вирішують дану проблему негативно. Відповідно до іншої точки зору, істинними інсиденталомами — метастазами можуть вважатися утворення, виявлені в осіб із первинною, раніше недіагностованою пухлиною. В онкологічних хворих до 50–70 % інсиденталом НЗ виявляються метастазами. Набагато рідше (2,1–5,8 %) інсиденталоми виявляються метастазами окультних злоякісних пухлин інших локалізацій. За частотою ураження метастазами НЗ посідає сьоме місце серед інших органів. Найчастіше в неї метастазують рак молочної залози, легень, печінки, лімфома, меланома, рідше — пухлини нирки, товстого кишечника [33].
Очевидно, слід вважати обґрунтованою точку зору, що якщо у хворого з онкологічним анамнезом виявляється утворення в НЗ, його слід насамперед розглядати як метастаз і вживати заходів для пошуку інших метастазів або рецидиву пухлини. У разі виявлення утворення з ознаками злоякісності за даними топічної діагностики у хворого без онкологічного анамнезу є більше підстав припускати, що воно є первинним раком НЗ або, набагато рідше, метастазом недіагностованої пухлини іншої локалізації.
Тут доречно буде згадати ще про один метод діагностики інсиденталом НЗ — пункційну біопсію. Основним показанням для її застосування є виявлення додаткового утворення в НЗ у хворого з онкологічним анамнезом за відсутності системного метастазування. Пунктувати рекомендується утворення розміром понад 2,0 см. Багато дослідників підкреслюють труднощі цитологічного розмежування доброякісних і злоякісних новоутворень НЗ, але метастази пухлин інших локалізацій у надниркову залозу можуть бути чітко диференційовані від первинних адреналових пухлин. Пункційна біопсія є досить складним дослідженням і може супроводжуватися серйозними ускладненнями. Перед її проведенням обов’язково слід виключити наявність феохромоцитоми. Виконується біопсія пункції під контролем УЗД або КТ досвідченим фахівцем.
Серед інших видів інсиденталом, які становлять меншість у структурі даної категорії утворень, найчастіше спостерігаються ліпоми і мієлоліпоми, далі — кісти, псевдокісти, гематоми і, нарешті, рідкісні типи пухлин і псевдопухлинних утворень. Більшість із них мають певні характеристики, які виявляються при топічній діагностиці; опис їх міститься у відповідних розділах. Однак їх наявність не виключає необхідності проведення спеціальних гормональних і додаткових досліджень за показаннями з подальшою оцінкою їх значимості та прийняттям рішення щодо тактики. Окремо слід згадати про псевдоадреналові утворення, які можуть імітувати справжню патологію НЗ. Диференціація їх нерідко буває доволі складною, а частота виявлення і правильна інтерпретація залежать від кваліфікації дослідника.
Виявивши інсиденталому НЗ, виконавши перерахований вище комплекс досліджень і встановивши клінічний діагноз, слід розв’язати основне питання: оперувати чи обмежитися спостереженням? Показаннями для оперативного лікування слід вважати:
— усі випадки гормоносекретуючих інсиденталом, незалежно від їх розмірів і того, чи є вони доброякісними або злоякісними; для хворих з ознаками автономної гіперсекреції кортизолу (субклінічний синдром Кушинга) питання про операцію вирішується індивідуально;
— інсиденталоми з ознаками злоякісності, метастази в НЗ за відсутності системного метастатичного ураження або рецидиву первинної пухлини;
— доброякісні інсиденталоми розміром понад 4,0 см; слід виділити інтервал «сірої шкали» — 4,0–6,0 см, коли рішення про операцію приймається індивідуально;
— доброякісні інсиденталоми, під час спостереження за якими відмічаються збільшення розмірів, поява ознак злоякісності, гормональної активності;
— інші пухлини і пухлиноподібні утворення, якщо вони досягають значних розмірів, мають ознаки злоякісності і супроводжуються клінічною симптоматикою.
Приймаючи рішення про оперативне лікування, хірург повинен враховувати клінічний діагноз — яка саме нозологічна форма адреналової патології підлягає операції. Втручання з діагнозом «інсиденталома НЗ» неприпустимі і є грубою помилкою, що свідчить про низьку кваліфікацію хірурга. Оптимальною операцією для більшості подібних пухлин є лапароскопічна адреналектомія з пухлиною. Відкриті операції показані для злоякісних пухлин значних розмірів, особливо з ознаками інвазії в навколишні структури.
З огляду на те, що більшість інсиденталом НЗ є доброякісними утвореннями, не менш важливим є визначення щодо них подальшої тактики — режим і тривалість спостереження, порядок й обсяги виконання контрольних клініко-гормональних і візуалізуючих досліджень, принципи оцінки отриманих результатів. У низці настанов вказується, що за наявності гормонально-неактивних аденом без ознак злоякісності розміром менше 3–4 см подальше спостереження не показане. Відзначається, що в подібних пухлинах вкрай рідко спостерігається тенденція до росту, озлоякіснення, появи гормональної активності. В інших випадках, особливо при найменших сумнівах первинних результатів, рекомендуються контрольні обстеження через 3, 6, 12 місяців і потім через 1–2 роки, максимальний термін встановлюється до п’яти років. Дані параметри є предметами обговорення в різних клініках.
Наведені в даній роботі показники лише частково свідчать про значущість проблеми інсиденталоми НЗ, що обґрунтовано могла б стати предметом подальшого висвітлення в серії статей.
Конфлікт інтересів. Автор заявляє про відсутність конфлікту інтересів та власної фінансової зацікавленості при підготовці даної статті.
Отримано/Received 02.02.2021
Рецензовано/Revised 24.02.2021
Прийнято до друку/Accepted 02.03.2021

/59.jpg)