Резюме
Мета дослідження: розробити показання до хірургічного лікування хворих iз грижами стравохідного отвору діафрагми (ГСОД) і оцінити його результати. Матеріали та методи. У відділенні хірургії органів травлення ДУ «Інститут гастроентерології НАМН України» за період 2017–2019 рр. обстежено і прооперовано 45 пацієнтів iз грижами стравохідного отвору діафрагми. Віддалені результати лікування вивчені в терміни від 6 міс. до 2 років у 19 (42,2 %) хворих. Результати. У наших дослідженнях серед 45 оперованих пацієнтів у 27 (60,0 %) діагностовано аксіальну ГСОД (тип I), у 9 (20,0%) — параезофагеальну ГСОД (тип II), у 8 (17,8 %) — змішану ГСОД (тип III), в 1 (2,2 %) — вкорочення стравоходу (тип IV). Гігантські ГСОД, що потребуюсь алопластики, спостерігалися у 8 (17,8 %) хворих, вкорочення стравоходу на тлі великих ГСОД з несформованою стриктурою нижньої третини стравоходу діагностовано в 1 (2,2 %) пацієнта. Крурорафію виконано всім хворим: задню — в 24 (53,3 %) випадках, передню і задню — в 13 (28,9 %), алопластику — у 8 (17,8 %). Проведено лапароскопічні фундоплікації: за Нiссеном — у 36 (80,0 %) пацієнтів, за Тупе — в 6 (13,3 %), за Дором — у 3 (6,7 %). Летальних випадків не було. Середня тривалість втручання становила (135 ± 24) хв, середній час фіксації трансплантата — (24 ± 12) хв. Висновки. Лапароскопічні антирефлюксні операції є високоефективними в лікуванні ГСОД, добре переносяться і характеризуються невеликою частотою ускладнень (6 (13,3 %) випадків), швидким відновленням хворих у післяопераційному періоді, що дозволяє визнати їх операціями вибору в лікуванні цієї патології. Вибір методу хірургічного втручання при ГСОД визначається особливостями анатомічних відношень та завданнями відновлення стравохідно-шлункового переходу і діафрагми.
Цель исследования: разработать показания к хирургическому лечению больных с грыжами пищеводного отверстия диафрагмы (ГПОД) и оценить его результаты. Материалы и методы. В отделении хирургии органов пищеварения ГУ «Институт гастроэнтерологии НАМН Украины» за период 2017–2019 гг. обследовано и прооперировано 45 пациентов с грыжами пищеводного отверстия диафрагмы. Отдаленные результаты лечения изучены в сроки от 6 мес. до 2 лет у 19 (42,2 %) больных. Результаты. В наших исследованиях среди 45 оперированных пациентов у 27 (60,0 %) диагностирована аксиальная ГПОД (тип I), у 9 (20,0 %) — параэзофагеальная ГПОД (тип II), у 8 (17,8 %) — смешанная ГПОД (тип III), у 1 (2,2 %) — укорочение пищевода (тип IV). Гигантские ГПОД, требующие аллопластики, наблюдались у 8 (17,8 %) больных, укорочение пищевода на фоне больших ГПОД с формирующейся стриктурой нижней трети пищевода диагностировано у 1 (2,2 %) пациента. Крурорафия выполнена всем больным: задняя — в 24 (53,3 %) случаях, передняя и задняя — в 13 (28,9 %), аллопластика — в 8 (17,8 %). Проведены лапароскопические фундопликации: по Ниссену — у 36 (80,0 %) пациентов, по Тупе — у 6 (13,3 %), по Дору — у 3 (6,7 %). Летальных исходов не было. Средняя продолжительность вмешательства составила (135 ± 24) мин, среднее время фиксации трансплантата — (24 ± 12) мин. Выводы. Лапароскопические антирефлюксные операции являются высокоэффективными в лечении ГПОД, хорошо переносятся и характеризуются небольшой частотой осложнений (6 (13,3 %) случаев), быстрым восстановлением больных в послеоперационном периоде, что позволяет признать их операциями выбора в лечении данной патологии. Выбор метода хирургического вмешательства при ГПОД определяется особенностями анатомических взаимоотношений и задачами восстановления пищеводно-желудочного перехода и диафрагмы.
Background. The purpose was to develop indications for surgical treatment of patients with hiatal hernias and evaluate its results. Materials and methods. At the Department of Surgery of Digestive Organs of SI “Institute of Gastroenterology of the National Academy of Medical Sciences of Ukraine”, 45 patients with hiatal hernias were examined in 2017–2019. Long-term treatment results were studied within 6 months to 2 years in 19 (42.2 %) individuals. Results. In our studies, among 45 operated patients, 27 (60.0 %) had a diagnosis of axial hiatal hernia (type I), 9 (20.0 %) — paraesophageal hiatal hernia (type II), 8 (17.8 %) — combined hiatal hernia (type III), 1 (2.2 %) patient had hiatal hernia with a shortening of the esophagus (type IV). Grade I of hiatal hernia was noted in 25 (55.6 %) people, grade II occurred in 12 (26.7 %), and grade III, when body and even the antral part of the stomach prolapse into the posterior mediastinum, — in 8 (17.8 %) patients. Cruroplasty was performed in 100 % of cases: posterior — in 24 (53.3 %) individuals, anterior and posterior (сombined) — in 13 (28.9 %), alloplasty — in 8 (17.8 %). Laparoscopic fundoplication was carried out in all patients: Nissen fundoplication — in 36 (80.0 %), Toupet fundoplication — in 6 (13.3 %), Dor fundoplication — in 3 (6.7 %). There were no fatal cases. The average duration of surgery was (135 ± 24) min, the average time of transplant fixation — (24 ± 12) min. Conclusions. Therefore, laparoscopic antireflux operations are highly effective in the treatment of hiatal hernias, well tolerated and characterized by a low percentage of complications (6 (13.3 %) cases), rapid recovery of patients in the postoperative period, allowing them to be recognized as surgery of choice in the treatment of this pathology. The choice of surgical procedure for hiatal hernia is determined by the features of anatomical interrelations and the purpose of restoring the esophageal-gastric junction and diaphragm.
Introduction
Hiatal hernia (HH) and gastroesophageal reflux disease are some of the most common pathologies in modern gastroenterology (second or third place in the structure of gastrointestinal diseases), along with such diseases as chronic cholecystitis and peptic ulcer of the stomach and duodenum [10]. In a targeted examination, HH is detected in 1–9 % of observations, and among the elderly — in 50 % of cases [3]. The detection rate of HH varies from 3 to 33 % and reaches 50 % in the elderly. HH accounts for 98 % of all diaphragm hernias, and in 50 % of cases does not cause any clinical manifestations and is not diagnosed [1, 2, 7].
HH plays a leading role in the development of incompetence of the lower esophageal sphincter (LES) and pathological gastrointestinal reflux [5, 6]. The only radical way to restore the size of the hiatus and the function of the cardiac sphincter with correction of gastroesophageal reflux is surgery. In this regard, the assessment of the main diagnostic criteria of the ATCM and the technical features of the operations is of great importance.
Minimally invasive interventions have changed the ratio of surgeries for HH and have significantly expanded the indications for surgical treatment. The main aim of surgical treatment is correction of anatomical and physiological disorders: the repair of diaphragmatic hernia, the correction of antireflux function of the LES due to fundoplication and cruroplasty, providing free antegrade passage of food [4, 8]. Despite many years of experience in laparoscopic surgery for HH, many issues are debated, remain relevant and require practical solutions [9, 10].
In our study, the combined use of clinical and instrumental methods allowed us to identify the most important features that influence the choice of cruroplasty with the strengthening of the hiatal perimeter and the choice of the method of antireflux reconstruction, which was determined by the severity of reflux manifestations and the contractile activity of the esophagus. Thus, the rationale for surgical tactics consisted of preoperative and intraoperative criteria.
Purpose: to develop indications for surgical treatment of patients with hiatal hernias and evaluate its results.
Materials and methods
At the Department of Surgery of Digestive Organs of SI “Institute of Gastroenterology of the National Academy of Medical Sciences of Ukraine”, 45 patients with hiatal hernias were examined in 2017–2019: 26 (57.9 %) women and 19 (42.2 %) men whose average age was (43.2 ± 12.6) years. Long-term treatment results were studied within 6 months to 2 years in 19 (42.2 %) patients.
To establish and confirm the diagnosis, patients underwent radiography of the esophagus, stomach, and duodenum. It consisted of examination radiography and X-ray with the use of barium sulfate (ATC code VO8BF02) on the apparatus OPERAT90SEX. Special methods and techniques were used to detect the incompetence of the esophageal-gastric junction. Polypositional radiography was performed in the vertical, horizontal, and Trendelenburg position of the patient, at the time of lifting the apparatus, with forced breathing. One of the main instrumental research methods in the study of esophagogastroduodenal pathology was esophagogastroduodenoscopy (EGDS). EGDS were performed at the Department of Minimally Invasive Endoscopic Interventions and Instrumental Diagnosis of the Institute using the Olympus GIF-Q20 fibrogastroscope (Japan) and the Pentax EG-290Kp (Japan) videogastroscope.
To study the esophageal motility and the pressure at the level of the LES, as well as to control the state of the formed fundoplication cuff, esophageal manometry was used. The tests are performed with the use of the original device for studying the gastrointestinal motility — MNH-01 (protected by certificate of authorship No. 923521 “Device for the study of motility of a biological object”, published on 30.04.82, Bulletin No. 16 and certificate for the promo version No. 12575), manufactured by Ukrainian Medical Systems company. The selection of patients for laparoscopic surgery was performed taking into account the following indications: the diagnosis of the hernia was established radiographically and according to EGDS with the presence of complications (esophagitis, erosion and esophageal ulcers, bleeding), relapse after surgical treatment of HH.
Results and discussion
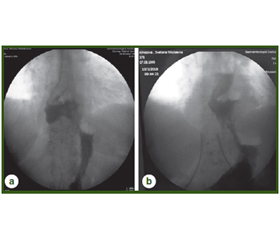
The most important was the radiological examination, which allowed obtaining all the changes in the anatomical correlation between the esophagus, stomach, and diaphragm. Among 45 operated patients, 27 (60.0 %) were diagnosed with axial HH (type I), 9 (20.0 %) — with paraesophageal HH (type II), 8 (17.8 %) — combined HH (type III), 1 (2.2 %) patient had HH with a shortened esophagus (type IV). Grade I of HH was found in 25 (55.6 %) patients, grade II — in 12 (26.7 %) and grade III, when body and even the antral part of the stomach prolapse into the posterior mediastinum, was diagnosed in 8 patients (17.8 %) (Fig. 1).
Giant hernias requiring alloplasty were observed in 8 (17.8 %) patients, of whom 1 (2.2 %) had esophageal shortening with unformed stricture of the lower third of the esophagus (Fig. 2).
/43_2.jpg)
Gastroesophageal reflux and pressure reduction at the LES level are important factors that influence the choice of antireflux reconstruction. In patients with HH, the pressure averaged (14.7 ± 3.9) mm Hg. When moving the balloon from the stomach to the esophagus, the pressure peak was not observed in 22.0 % of the examined patients, in 34.4 % it did not exceed 10 mm Hg, in 43.8 % of individuals the pressure peak at anatomical narrowing was more than 10 mm Hg. During endoscopic examination, the erosions of the lower third of the esophagus were identified in 8 (17.8 %) patients. According to the Los Angeles classification, 3 (67 %) patients had grade A esophagitis, and 5 (11.1 %) had grade B. The average pressure in the balloon at the level of the cardioesophageal sphincter was (14.7 ± 3.9) mm Hg, indicating that cardiac function was impaired. The decreased pressure in the esophagocardial zone led to the disruption of the locking function of the LES, resulting in esophageal manifestations of gastroesophageal reflux disease.
According to the laboratory data, anemia was observed in 4 (8.8 %) patients with axial (cardiofundal and subtotal) hernias.
When establishing a diagnosis of HH and the presence of complications (esophagitis, esophageal erosion, anemia, bleeding, large HH with fixation in the hernia gate, postoperative relapses), indications for surgical intervention were developed. So, in the preoperative period, indications for surgical treatment were functional or organic manifestations of reflux against the background of radiological, endoscopic and manometric signs of HH.
The main aims of surgical operation are: repair of diaphragmatic hernia and restoration of the enlarged esophageal hiatus by сruroplasty or meshes with correction of the antireflux function of the LES due to symmetrical fundoplication, restoration of the His angle, mobilization of the intra-abdominal portion of the esophagus (at least 4 cm), providing antegrade passage of the food. The steps for performing the intervention are shown in Fig. 3.
An important factor in the normal function of the LES is the length of the abdominal esophagus. We believe that if the length of the abdominal part of the LES is less than 1 cm, then the risk of developing reflux increases significantly, regardless of the pressure in it. Therefore, the segment of the abdominal part of the esophagus is isolated from adhesions at a distance of at least 4 cm (Fig. 4).
The choice of the method for antireflux reconstruction was determined by the severity of reflux manifestations and the contractile activity of the esophagus. With normokinesia of the esophagus and pronounced manifestations of reflux, “floppy” Nissen reconstruction was performed with complete mobilization of the fundus and dissection of the gastrosplenic and esophageal-diaphragmatic ligaments. With minimal manifestations of reflux or impairment of the LES motility, anatomical features, partial circular or anterior fundoplications were performed (A. Toupet, D. Dor) (Fig. 5b, c).
The main problem of surgery for HH is the correction of the size of the esophageal hiatus. To prevent re-dislocation of the gastroesophageal junction to the mediastinum with structural inferiority of diaphragmatic branches or if the size of the esophageal hiatus was more than 20 cm2, we used prosthetic materials in our work. With small sizes of esophageal hiatus and full value diaphragmatic branches, the posterior or posterior and anterior cruroplasty with fundodiaphragmopexy was performed.
Large and gigantic HH were diagnosed in 11 (24.4 %) patients. The inability to approach the diaphragmatic branches and perform cruroplasty served an indication for the use of mesh in 8 (17.8 %) people. In our work, we used a lightweight polytetrafluoroethylene mesh with a peripheral nitinol frame and MMDI (USA) mesh (Fig. 6, 7).
Thus, it is possible to distinguish intraoperative criteria that affect the tactics of surgical treatment:
1) increased distance between the diaphragmatic branches, thinning of the diaphragmatic branches due to dystrophic processes;
2) diameter of HH;
3) location of cardia, fundus, body of the stomach above the hiatus;
4) dislocation of the abdominal part of the esophagus;
5) shortening, stenosis of the esophagus.
Type of operations in patients with HH (n = 45):
1. Cruroplasty:
— posterior — 24 (53.3 %);
— anterior and posterior — 13 (28.9 %);
— repair, fixation of allotransplant MMDI, Bard — 8 (17.8 %)
2. Fundoplication:
— Nissen fundoplication — 36 (80 %);
— Toupet fundoplication — 6 (13.3 %);
— Dor fundoplication — 3 (6.7 %).
3. Fundodiaphragmopexy — 34 (75.6 %).
There were no fatal cases. Pneumothorax occurred in 2 patients (4.4 %), bleeding from the spleen capsule — in 2 (4.4 %). The average duration of surgery was (135 ± 24) min, the average time of transplant fixation — (24 ± 12) min.
The efficiency of the treatment in the studied patients was evaluated according to the following criteria:
1. Clinical disappearance of heartburn, belching, regurgitation, epigastric pain.
2. The absence of erosions in the lower third of the esophagus, the absence of prolapse of the gastric mucosa into the esophagus according to data of endoscopy.
3. The absence of prolapse of a part of the stomach to the thorax, the absence of sphincter incompetence, the absence of gastric mucosal prolapse according to data of X-ray examination.
4. Normalization of pressure in the LES according to manometry.
When studying the long-term results (up to 6 months), relapses of the HH were detected in 6 (13.3 %) patients. In 1 case, the cause of relapse was signs of a shortened esophagus, making it difficult to form an antireflux cuff. In one patient with large HH, the fixation of the allotrasplant behind the diaphragmatic branches provoked the eruption of sutures. In 2 cases, relapse of the HH was associated with the technical aspects of surgical treatment.
So, in the preoperative period, functional or organic manifestations of gastroesophageal reflux on the background of radiological, endoscopic, and manometric signs of the hernia were indications for surgical treatment of patients with HH. In case of the LES dysfunction, gastroesophageal reflux and pressure reduction at the level of (14.7 ± 3.9) mm Hg are important factors influencing the choice of antireflux reconstructions. The main aims of surgical treatment are repair of diaphragmatic hernia, restoration of the enlarged esophageal hiatus by cruroplasty or mesh with correction of the antireflux function of the LES due to symmetrical fundoplication, restoration of the angle of His, mobilization of intraperitoneal portion of the esophagus (at least 4 cm), providing free antegrade passage of food.
Indications for using meshes are structural inferiority and the impossibility of approaching the diaphragmatic branches, distance between them of more than 3 cm, the diameter of the esophageal hiatus over 5 cm. Developed intraoperative criteria influence surgical treatment in patients with HH: increased distance between the diaphragmatic branches, thinning of the branches due to dystrophic processes, the diameter of the esophageal hiatus, the location of the cardia, fundus and body of the stomach relative to the hiatus, the location of the abdominal part of the esophagus, the shortening or stenosis of the esophagus.
Conclusions
Thus, laparoscopic antireflux operations are highly effective in the treatment of HH, well tolerated and characterized by a low percentage of complications (6 (13.3 %) cases), rapid recovery of patients in the postoperative period, which allows them to be recognized as the surgeries of choice in the treatment of this pathology. The choice of the method of surgical intervention in case of HH is determined by the features of anatomical interrelations and the purpose of restoring the esophageal-gastric junction and diaphragm.
Conflicts of interests. Authors declare the absence of any conflicts of interests and their own financial interest that might be construed to influence the results or interpretation of their manuscript.
Information about funding. The work was carried out as a part of the research work of the SI “Institute of Gastroenterology of the National Academy of Medical Sciences of Ukraine”.

/43.jpg)
/44.jpg)
/45.jpg)