Резюме
Актуальність. Невирішеними питаннями застосування лазеріндукованої інтерстиціальної термотерапії (ЛІТТ) у лікуванні солідних вузлів щитоподібної залози (ЩЗ) на сьогодні є визначення показань і протипоказань, методики і технології її виконання, підвищення ефективності і покращання віддалених результатів. Мета дослідження: вивчити вплив ЛІТТ на навколовузлову тканину і функціональну здатність ЩЗ, визначити фактори, що впливають на терміни заміщення вузла сполучною тканиною та її об’єм, розробити показання до повторного застосування термотерапії. Матеріали та методи. З використанням ЛІТТ проліковані 272 хворі на вузловий зоб без ознак кістозної дегенерації. Усі пацієнти — жінки віком від 22 до 68 років. Об’єм вузлів був у межах від 0,8 до 5,0 см3. За ультразвуковими характеристиками, зокрема за ехогенністю, вузли були такими: 46 — гіпоехогенні, 189 — ізоехогенні та 37 — гіперехогенні. Використовували діодний лазер Лахта-Мілон. ЛІТТ проводили за таких параметрів: довжина хвилі 1060 нм, безперервний режим, потужність випромінювання у межах від 2,5 до 3,2 Вт. Перебіг ЛІТТ контролювали сонографічно. Зміни у вузлі, навколовузловій тканині та функцію залози після ЛІТТ визначали на другу добу, через 2 тижні, через 1, 3, 6, 9 та 12 місяців після маніпуляції. Результати. На другу добу після лазерної термотерапії у вузлах розвивається асептичне запалення, а розміри їх збільшуються на 25–30 %. У подальшому, у визначені терміни обстеження, розміри вузлів зменшувались, показники гормональної функції не змінювались. Через 6 місяців після ЛІТТ при розмірах вузлів до 2 см повне їх заміщення сполучною тканиною відмічалось у всіх випадках гіпо- й ізоехогених вузлів і в 71 % — гіперехогенних, а при розмірах від 2 до 5 см — у 75 % випадків вузлів гіпоехогенної структури, 18 % — ізоехогенної і не було позитивного ефекту у разі гіперехогенних вузлів. У випадках неефективного лікування знадобилося проведення повторної ЛІТТ, після якої у всіх пацієнтів настала повна редукція вузла. Висновки. У розроблених режимах ЛІТТ не викликає деструктивних змін у навколовузловій тканині і розладів гормональної функції залози. Тривалість регресу і заміщення вузла сполучною тканиною визначають його ехогенність і об’єм. Показаннями до повторного застосування термотерапії є залишкова тканина в ділянці вузла в межах більше 42 % від вихідного об’єму через півроку після проведеного лікування та наявність у ній тиреоїдного епітелію.
Актуальность. Нерешенными вопросами применения лазериндуцированной интерстициальной термотерапии (ЛИТТ) в лечении солидных узлов щитовидной железы (ЩЖ) на сегодняшний день являются определение показаний и противопоказаний, методики и технологии ее выполнения, повышение эффективности и улучшение отдаленных результатов. Цель исследования: изучить влияние ЛИТТ на околоузловую ткань и функциональную способность ЩЖ, определить факторы, влияющие на сроки замещения узла соединительной тканью и ее объем, разработать показания к повторному применению термотерапии. Материалы и методы. С использованием ЛИТТ пролечены 272 больных узловым зобом без признаков кистозной дегенерации. Все пациенты — женщины от 22 до 68 лет. Объем узлов был в пределах от 0,8 до 5,0 см3. По ультразвуковым характеристикам, в частности по эхогенности, узлы были такими: 46 — гипоэхогенные, 189 — изоэхогенные и 37 — гиперэхогенные. Использовали диодный лазер Лахта-Милон. ЛИТТ проводили по таким параметрам: длина волны 1060 нм, непрерывный режим, мощность излучения в пределах от 2,5 до 3,2 Вт. Течение ЛИТТ контролировали сонографически. Изменения в узле, околоузловой ткани и функцию железы после ЛИТТ определяли на вторые сутки, через 2 недели, через 1, 3, 6, 9 и 12 месяцев после манипуляции. Результаты. На вторые сутки после лазерной термотерапии в узлах развивается асептическое воспаление, а размеры их увеличиваются на 25–30 %. В дальнейшем, в определенные сроки обследования, размеры узлов уменьшались, показатели гормональной функции не изменялись. Через 6 месяцев после ЛИТТ при размерах узлов до 2 см3 полное замещение их соединительной тканью отмечалось во всех случаях гипо- и изоэхогенных узлов и в 71 % — гиперэхогенных, а при размерах от 2 до 5 см3 — в 75 % случаев узлов гипоэхогенной структуры, в 18 % — изоэхогенной и не было положительного эффекта при гиперэхогенных узлах. В случаях неэффективного лечения потребовалось проведение повторной ЛИТТ, после которой у всех пациентов наступила полная редукция узла. Выводы. В разработанных режимах ЛИТТ не вызывает деструктивных изменений околоузловой ткани и гормональной функции железы. Продолжительность регресса и замещение узла соединительной тканью определяют его эхогенность и объем. Показаниями к повторному применению термотерапии являются остаточная ткань в узле в пределах более 42 % от исходного объема через полгода после проведенного лечения и наличие в ней тиреоидного эпителия.
Background. Indications and contraindications, methods and technologies of implementation, increased efficiency and improved long-term results are the unresolved issues when using laser-induced interstitial thermotherapy (LITT) in the treatment of solid thyroid nodules. Objective: to study the effect of LITT on parathyroid tissue and functional capacity of the thyroid gland, to determine the factors affecting the time of replacement by connective tissue and its volume; to develop indications to repeated thermotherapy. Materials and methods. Using the LITT we treated 272 patients with a nodular goiter with no signs of cystic degeneration. All patients — women aged 22 to 68 years. The size of nodules was within the range of 0.8 to 5.0 cm3. In terms of ultrasonic characteristics, in particular echoicity, the nodules were as follows: 46 — hypoechoic, 189 — isoechoic and 37 — hyperechoic. We used a diode laser Lakhta-Milon. LITT was performed on such parameters: the wave length 1060 nm, continuous operation, output power ranging from 2.5 to 3.2 W. LITT was controlled by ultrasound. Changes in the nodule, parathyroid tissue and gland function after LITT was determined on day 2, as well as 1, 3, 6, 9 and 12 months after the procedure. Results. An aseptic inflammation occurred on the second day after laser thermotherapy in nodules, and their size increased by 25–30 %. Later, in a certain period of the survey, the size of nodules decreased, rates of hormonal function did not change. Six months after the LITT, with nodule size up to 2 cm3, a complete replacement by connective tissue occurred in all cases of hypo- and isoechoic nodules and in 71 % — of hyperechoic, and with sizes from 2 to 5 cm3 — in 75 % of hypoechoic structures, 18 % of isoechoic, and there was no beneficial effect in hyperechoic nodules. If the treatment failed, repeated LITT was required, after which all patients had complete reduction of the nodule. Conclusions. In the developed modes, the LITT did not cause destructive changes in parathyroid tissue and hormonal gland function. Duration of regression and replacement of the nodule by connective tissue is determined by its echogenicity and size. The residual tissue in the nodule within more than 42 % of the initial size in six months after the treatment and the presence of thyroid epithelium in it are the indications for re-use of thermotherapy.
Introduction
Nowadays, it is generally recognized that since the detection of nodular goiter before the indications for surgical treatment the effective methods of conservative therapy do not exist [1, 2]. Since the 80th years of the last century, the technique of sclerotherapy of nodules has been used in the treatment of this pathology. However, it has a number of significant disadvantages and complications: the regression size of the nodule does not exceed 50 %, there is destruction of paranodular tissue, severe pain syndrome.
Since 1998, the technique of laser-induced interstitial thermotherapy (LITT) has been developed and implemented in the treatment of solid nodules of the thyroid gland [3–5]. Today, it is widely used in America, Wes–tern Europe, Russia, Asia and Japan. However, despite the widespread use of this method and the experience gained, the issues of indications and contraindications, the methodology and technology of its implementation, the increase of efficiency and improvement of the treatment results [6–8] are disputing and still unresolved.
The purpose of the work. Studying the effect of LITT on the nodular surrounding tissue and the functional capacity of the thyroid, determining the factors that influence the timing of the nodule replacement with the connective tissue and its size, to developing the indications for the re-use of thermal therapy.
Materials and methods
LITT was used as an independent method for the treatment of clinically significant, solitary euthyroid and toxic, solid nodules. 272 patients were treated, among whom there were 225 patients with solid and heterogeneous nodules with euthyroid function and 47 patients with heterogeneous autonomously functioning nodules and clinical manifestations of thyrotoxicosis. All patients were women aged 22 to 68 years. Before treatment, the following examinations were performed: ultrasonography of the nodules and nodular surroun–ding tissue, nodule puncture biopsy from three points with subsequent cytological examination, determination of thyroid stimulating hormone (TSH), thyro–xine (T4), calcitonin, thyroid peroxidase autoantibodies (TPOAb), common blood and urine tests, duration of bleeding and coagulation time, blood test for infection (syphilis, hepatitis).
The size of nodules was in the range of 0.8 to 5.0 cm3. In 158 cases, it did not exceed 2 cm3, and in 114 patients — from 2 to 5 cm3. According to the ultrasound characteristics, in particular, the echogenicity of the nodules were as follows: 46 — hypoechoic, 189 — isoechoic and 37 — hyperchoic (table 1). In patients with hyperfunctional nodules, blood flow through the nodule was strengthened. The fraction of the uninfected by nodular tissue of the thyroid (outside the nodular parenchyma), was determined by the formula in cm3: Vr = Vt – Vn; where Vr is the size of residual tissue, Vt — size of the thyroid, and Vn — size of the nodule. In 149 patients, the residual gland tissue was > 80 %, in 96 patients — from 80 to 60 % and in 27 — in the range of 60–55 %.
Lakhta-Milon diode laser was used. LITT was performed according to the following parameters: wavelength 1060 nm, continuous mode, radiation power in the range from 2.5 to 3.2 W. The course of LITT was monitored sonographically.
Changes in the nodule, nodular tissue and the function of the gland after LITT were determined on the second day in 2 weeks, in 1, 3, 6, 9 and 12 months after manipulation. The changes in the size of nodules and their structure were studied using the ultrasound device “TOSHIBA” Nemio XG SSA-580 A, levels T4, TSH and TPOAb (immune enzyme method), morphological changes in punctates from the nodule site were conduc–ted in cases of incomplete reduction in 9 months after LITT and in 6 months after the repeated LITT.
The efficacy of LITT at the control treatment stages was evaluated by the percentage of nodule regression compared with the baseline data. Finished treatment was considered to be cases of complete nodular tissue substitution to the connective tissue.
Contraindications to the LITT were considered to be the size of a nodule of more than 10 cm3, the percentage of tissue fraction of the gland without a nodule was less than 40 % of the fraction size.
Results
On the second day after LITT the size of nodules was increased on 20–35 % compared to the initial data. The percentage of their increase depended on echogenicity. Hyperechoic nodules were increased on 20–25 %, isoechoic — on 25–30 %, and hypoechoic — on 25–35 %. An increase in the size of nodules is a consequence of aseptic inflammation and tissue edema within the nodule. In cytological examination of nodular tissues, signs of aseptic inflammation (leukocytic infiltration, edema of interstitial tissue) were revealed. There are no signs of inflammation in paratodial tissue punctures. The indices of TPOAb, TSH, and T4 did not differ significantly from the original values (p > 0.05).
Two weeks after the treatment, according to the ultrasound examination, the size of nodules decreased to baseline (before treatment) and their echogenicity did not change. The levels of TPOAb, TSH and T4 were within normal limits.
One month after treatment, the reduction in the size of nodules ranged from 28 to 42 % (32.0 ± 0.4 %, p < 0.01) and was different depending on echogenicity. So, hyperechoic nodules decreased on average on 28–30.0 %, and iso- and hypoechoic — on 31–42 %. In the cytological study, fibrous transformation was determined in the tissue of the nodules, and in a part of all patients, mainly with a baseline of nodules greater than 2 cm3, in addition, there were signs of aseptic inflammation or swelling of the interstitial tissue. In paranodular parenchyma, pathomorphological changes were absent. Indicators of antibodies to the microsomal fraction, levels of TSH and thyroxin were within normal limits and compared with the data at the second week after LITT did not significantly change (p > 0.05).
3 months after, 105 patients (38.6 %) noted complete replacement of the nodule with a connective tissue. Among them 102 patients had the size of the nodule before treatment less than 2 cm3 (hypoechoic — 28, isoechoic — 61, hypechoic — 13) and 3 patients — from 2 to 5 cm3, all isoechoic. In all these patients, changes in the functional activity of the gland were within the limits of euthyroidism and, compared to the indicators in a month, were not reliable (p > 0.05). The residual tissue volume in the nodule site was determined from 0.1 to 0.2 cm3, and the nodular size regress ranged from 84 to 92 %. In cytological examination of nodular site tissue there was a connective tissue. In the remaining 167 patients, the nodular size regress was in the range from 37 to 68 %.
For the sixth month of observation in 105 patients, who confirmed the replacement of nodules with connective tissue — the volume of a rumen did not change. Among the remaining 167 patients, 73 had sonographic signs of replacement of nodules with scar tissue, which size ranged from 0.2 to 0.4 cm3, and the reduction of the nodules size in comparison with the initial data was from 72 to 84 %. In the cytological study of the nodular site — connective tissue. Among these patients in 48 — the nodu–lar size before the LITT was less than 2 cm3, and by echogenicity — 2 hypoechoic, 39 isoechoic and 7 hyperechoic. In 25 ca–ses, the size of nodules was within the range of 2–5 cm3. Among them, there were 12 hypoechoic and 13 –isoechoic — 13. In general, 6 months after the LITT, replacement of nodules with connective tissue occurred in 178 patients (65.4 %), and the reduction of the nodular size was 72 to 92 %. In the remaining 94 patients, the reduction in the nodular size ranged from 41 to 58 %.
At the ninth month after the LITT there were no changes in the size of connective tissue in the site of no–dules. In 94 patients, the nodular size regression in comparison with the results for 6 months did not exceed 5 % and in general, compared with the baseline data, the reduction of nodules in these patients in the treatment process was in the range of 46 to 61 %. Before treatment in 8 of these patients the nodules were hyperechoic and in size less than 2 cm3; in 86 patients the nodules were from 2 to 5 cm3, and in 4 were hypoechoic, in 73 patients — isoechoic and 9 — hyperechoic and in 35 cases — functionally active. In the cytological study of the nodular site, a connective tissue and cells of the follicular epithelium of the thyroid gland were detected. All of these patients were retreated with LITT with a capacity of 3.0–3.2 W and a procedure duration from 10 to 15 minutes.
Three months after the repeated LITT, replacement of the nodule with connective tissue occurred in 55 patients. The residual size of nodules ranged from 0.4 to 0.6 cm3, and the regress compared with the initial size ranged from 73 to 76 %. In the rest 39 patients, the nodular size regression was in the range of 59 to 71 %.
At the sixth month of observation after repeated LITT in 55 patients in whom the replacement of nodules were confirmed with connective tissue, the rumen size did not change. In 39 patients, a sonographic picture of the parenchyma replacement of nodules with echosensitive tissue in the range of 0.45 to 0.6 cm3 was observed, and in the cytological study, there was a connective tissue without a thyroid epithelium. So, after repeated LITT, in all cases, replacement of nodular tissue with the connective tissue occurred.
Pathomorphological changes absence in different terms after LITT in nodular surrounding tissue, an increase above the norm in the level of blood antibodies to thyroid peroxidase, thyroid stimulating hormone and thyroxine suggests that the thermotherapy of the nodule using laser energy in selected modes does not cause parenchyma degeneration of the gland and disorders of its functional state.
Discussion
Our experience of using LITT in the treatment of solid thyroid nodules shows the high efficiency of this technique. Among 272 patients treated, the positive effect of treatment was achieved in all cases. The end result of treatment was the complete replacement of the nodule with the connective tissue. Among patients with autonomous functioning nodes 35 (74.5 %) of them required repeated LITT.
We believe that the factors that determine the effectiveness of LITT in the treatment of the nodular euthyroid goiter are the size and echogenicity of the nodule (table 2).
Nodules with initial size of up to 2 cm3 had a hig–her regression and a smaller size of rumen after LITT. The vast majority of these nodules was replaced on the connective tissue in 3–6 months after the LITT. The resi–dual rumen size did not exceed 12 % of the initial nodular size. The regression of nodules with an initial size of 2–5 cm3 was longer, and the size of residual tissue ranged from 15 to 40 %. These nodules required repeated LITT (table 2).
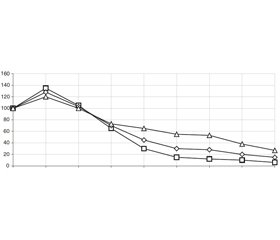
The echogenicity of nodules significantly influences the rate of their regression and size of residual scar. So, hypoechoic nodules reacted more intensely with size increase in 2 days after manipulation, regressed faster and replacement on the scar was observed in the interval of 3–6 months (p < 0.01). Nodules in the size from 2 to 5 cm3 and a part of hypechoic nodules in size up to 2 cm3 mostly required repeated LITT. The reactive edema of the isoechoic nodules was less pronounced and their replacement with the connective tissue was observed in the interval of 3–15 months after the LITT, and the residual size, that is, the size of the rumen, ranged from 9 to 28 % of the initial one. Hyperechoic nodules responded to LITT to the smallest extent by reactive edema and size increase, and the final size of the tissue at the site of the nodule was within the range of 15 to 36 % of the findings before treatment (fig. 1).
/58-1.jpg)
The nodule regression and the size of scar tissue did not depend on the age of patients and the percentage of unchanged tissue of the thyroid before treatment.
Indications for LITT re-use are considered to be delayed nodule regression, especially in the interval 6–9 months after treatment, reducing its size up to 58 %, in the presence of thyroid gland epithelium in residual tissue according to FNA.
Conclusions
1. In selected modes and technologies, laser-induced interstitial thermotherapy does not cause destructive changes in the nodular surrounding tissue and disorders of the thyroid gland function.
2. The result of laser-induced interstitial ther–motherapy is the complete replacement of the nodular tissue with the connective tissue. Its efficiency is 100 %.
3. Speed and completeness of nodular replacement with the connective tissue after laser-induced interstitial thermotherapy depend on the size and echogenicity of the nodules. In the size up to 2 cm3, the complete replacement tissue of hypo- and isoechoic nodules on the connective tissue occurred in all patients, and hype–rechoic — in 71 %. About 75 % of patients with 2 to 5 cm3 nodules required re-use of thermal therapy. This applies to all patients with hyperechoic nodules, 25 % — with hypoechoic and 82 % — isoechoic nodules.
4. Patients with residual tissue of the nodular formation require repeated thermotherapy. Absolute indications for its implementation are the slow reduction of the nodule, in the presence of nodular parenchyma among connective tissue elements.
Conflicts of interests. Author declares the absence of any conflicts of interests that might be construed to in–fluence the results or interpretation of their manuscript.
Список литературы
1. Gharib H., Papini E. Thyroid nodules: clinical importance, assessment, and treatment // Endocrinol. Metab. Clin. North Am. — 2007. — Vol. 36. — P. 707-35.
2. Gharib H., Papini E., Paschke R., Duick D.S., Valcavi R., Hegedüs L., Vitti P. AACE/AME/ETA Task Force on Thyroid Nodules American Association of Clinical Endocrinologists, Associazione Medici Endocrinologi, and European Thyroid Association Medical guidelines for clinical practice for the diagnosis and management of thyroid nodules: executive summary of recommendations // Endocr. Pract. — 2010. — Vol. 16. — P. 468-75.
3. Papini E., Rago T., Gambelunghe G., Valcavi R., Bizzarri G., Vitti P., De Feo P., Riganti F., Misischi I., Di Stasio E., Pacella C.M. Long-term efficacy of ultrasound-guided laser ablation for benign solid thyroid nodules. Results of a three-year multicenter prospective randomized trial // J. Clin. Endocrinol. Metab. — 2014. — Vol. 99(10). — P. 3653-9. — doi: 10.1210/jc.2014-1826.
4. Bandeira-Echtler E., Bergerhoff K., Richter B. Levothyroxine or minimally invasive therapies for benign thyroid nodules // Cochrane Database Syst. Rev. — 2014. — 6. — CD004098. — doi: 10.1002/14651858.CD004098.pub2.
5. Sui W.F., Li J.Y., Fu J.H. Percutaneous laser ablation for benign thyroid nodules: a meta-analysis // Oncotarget. — 2017. — Vol. 8(47). — P. 83225-83236. — doi: 10.18632/oncotarget.17928. eCollection 2017 Oct 10.
6. Initial report of the results of percutaneous laser ablation of benign cold thyroid nodules: evaluation of histopathological changes after 2 years / B. Cakir, E.S. Ugras, K. Gul et al. // Endocrine Patology. — 2009. — Vol. 20, № 3. — P. 170-176.
7. Treatment of benign cold thyroid nodules: a randomized clinical trial of percutaneous laser ablation versus levothyroxine therapy or follow-up / E. Papini, R. Guglielmi, G. Bizzarri et al. // Thyroid. — 2007. — Vol. 17(3). — P. 229-235.
8. Dossing H. Effect of ultrasound-guided interstitial laser photocoagulation on benign solitary solid cold thyroid nodules: one versus three treatments / H. Dossing, F.N. Bennedbaek, L. Hegedus // Thyroid. — 2006. — Vol. 16(8). — P. 763-768.

/56-1.jpg)
/57-1.jpg)