
Журнал «Здоровье ребенка» 4 (55) 2014
Вернуться к номеру
Clinical Paraclinical Parameters of Primary Arterial Hypertension in Adolescents
Авторы: Horlenko O.M., Sochka N.V., Debreceni O.V., Horlenko F.V., Piridi V.L., Tomey A.I., Debreceni K.O.,
Kossey G.B. - State Higher Educational Institution «Uzhgorod National University», Medical Faculty, Department of Pediatrics with Infectious Diseases, Uzhgorod
Рубрики: Педиатрия/Неонатология
Разделы: Клинические исследования
Версия для печати
We investigated children with primary arterial hypertension (PAH) from the Transcarpathian region of Ukraine (68 children, middle age 14.68 ± 0.84 years). In patients with arterial hypertension which PAH debuted in adolescence and have changes in lipid profile are formed pathological process in two ways: first way presented increase in total cholesterol associated with lower high-density lipoprotein (HDL) cholesterol indicators, and other is an increase in triglycerides with decreased levels of HDL cholesterol, according to data of M.M. Korenev et al. (2010, 2011). These changes in lipid profile is prognostically unfavorable signs of atherosclerosis which developed in the patients (1st way), in others — development of the metabolic syndrome in the young age (14–15 years), which we observed in our research. Our data are also relevant tendency. In children with PAH increase triglyceride levels (1.96 ± 0.04 mmol/l) associated with significant decrease in HDL cholesterol fraction (1.20 ± 0.31 mmol/l) which predicts development of the metabolic syndrome in the young age.
Ми досліджували дитячий контингент Закарпатської області з первинною артеріальною гіпертензією (ПАГ) (68 чол., середній вік — 14,68 ± 0,84 року). У тих хворих з артеріальною гіпертензією, у яких ПАГ дебютувала в підлітковому віці, спостерігаються зміни в ліпідному спектрі і патологічний процес формується у двох напрямках. Перший шлях представлений збільшенням рівня загального холестерину з більш низькими показниками фракції холестерину ліпопротеїдів високої щільності (ЛПВЩ). При другому шляху підвищення рівня тригліцеридів асоціюється зі зниженням рівня фракції холестерину ЛПВЩ, згідно з даними М.М. Коренева і співавт. (2010, 2011). Ці зміни в ліпідному спектрі є прогностично несприятливими для розвитку атеросклерозу (1-й шлях розвитку), у дітей із 2-м шляхом формування патологічного процесу очікується розвиток метаболічного синдрому в молодому віці (14–15 років), що і відзначено в нашому дослідженні. У дітей із ПАГ підвищення рівня тригліцеридів (1,96 ± 0,04 ммоль/л) асоційоване зі значним зниженням фракції холестерину ЛПВЩ (1,20 ± 0,31 ммоль/л), що відповідає прогнозу розвитку метаболічного синдрому в молодому віці.
Мы исследовали детский контингент Закарпатской области с первичной артериальной гипертензией (ПАГ) (68 чел., средний возраст — 14,68 ± 0,84 года). У тех больных с артериальной гипертензией, у которых ПАГ дебютировала в подростковом возрасте, наблюдаются изменения в липидном спектре и патологический процесс формируется в двух направлениях. Первый путь представлен увеличением уровня общего холестерина с более низкими показателями фракции холестерина липопротеидов высокой плотности (ЛПВП). При втором пути повышение уровня триглицеридов ассоциируется со снижением уровня фракции холестерина ЛПВП, согласно данным М.М. Коренева и соавт. (2010, 2011). Эти изменения в липидном спектре являются прогностически неблагоприятными для развития атеросклероза (1-й путь развития), у детей со 2-м путем формирования патологического процесса ожидается развитие метаболического синдрома в молодом возрасте (14–15 лет), что и представлено в нашем исследовании. У детей с ПАГ повышение уровня триглицеридов (1,96 ± 0,04 ммоль/л) ассоциировано со значительным снижением фракции холестерина ЛПВП (1,20 ±0,31 ммоль/л), что соответствует прогнозу развития метаболического синдрома в молодом возрасте.
children, primary arterial hypertension, parameters of homeostasis disorders.
діти, первинна артеріальна гіпертензія, параметри порушень гомеостазу.
дети, первичная артериальная гипертензия, параметры нарушений гомеостаза.
Статья опубликована на с. 39-42
Introduction
Primary arterial hypertension (PAH) comprises 90–95 % of the arterial hypertension in children. 66.0 % of people with hypertension have atherogenic changes in lipid profile, characterized by increased levels of total cholesterol, triglycerides, and have parallel decrease in fractions of antiatherogenic high-density lipoprotein (HDL) cholesterol. Arterial hypertension in the children is characterized by a large prevalence, has not only medical importance, but also social role. This disease is a major cause of morbidity and mortality of the adult population [1–3].
The Aim. To investigate the presentation parameters of children with PAH based on the study of levels of homeostasis and their correlation.
Materials and Methods
Clinical characteristic, laboratory study (clinical and biochemical blood tests, ELISA contents of interleukins 1, 6 in the blood serum), determining levels of hormones T4, thyroid-stimulating hormone (TSH), micro- and macroelements (phosphorus, potassium, calcium, sodium and chlorine) in the blood serum, statistics methods.
Results
We investigated children with PAH from Transcarpathian region (68 children, middle age 14.68 ± 0.84 years). The control group consisted of 30 healthy children, middle age 13.52 ± 0.22 years. We considered cli–nical manifestations of PAH in children.
Particularly representational signs in children with PAH were: palpitation (43.59 ± 5.65 %), headache (increased to the end of the day) (30.77 ± 5.26 %), pain in the heart area of short duration (28.21 ± 5.13 %), dizziness (orthostatic) (26.92 ± 5.05 %), as can be seen from Table 1.
We obtained the following data in the study of blood pressure (BP) in the children with PAH (Table 2).
SBP parameters significantly differed in studied children (125.12 ± 0.73 mmHg to 114.73 ± 0.58 mmHg, p < 0.05). Systolic hypertension 3–8 times prevails over diastolic in children according to the literature data. The prevalence of systolic hypertension in adolescence observed in all subgroups regardless of race, age and gender was found. This applies mainly to the PAH.
/40/40.jpg)
We also conducted biochemical blood serum tests (Table 3).
As shown in the Table 3, the children with PAH had significantly higher specific biochemical parameters, including total bilirubin (11.51 ± 0.49 mmol/l to 8.23 ± 1.02 mmol/l in children from the control group; p < 0.001). Revealed significant differences identified only in the levels of HDL (respectively 1.20 ± 0.31 mmol/l to 1.69 ± 0.01 mmol/l; p < 0.001) by following data. HDL is useful «antiatherogenic» factor which transferred of cholesterol from cells of peripheral organs (including arteries, arteries of the brain, etc.) to the liver where it will be excreted from the body in the form of bile acids. Elevated levels of total cholesterol were determined in 18.76 % of patients — up to 6.12 ± 0.21 mmol/l among children. These children have recorded violations in the increase of total cholesterol by fraction of LDL to 2.78 ± 0.42 mmol/l, when levels HDL fraction and TG were in the reference value. According to our investigation were found significant differences in the levels of cholesterol in children with PAH (2.35 ± 0.18 mmol/l to the control group — 0.84 ± 0.03 mmol/l). The rate of LDL more correlated with the risk of atherosclerosis than the total cholesterol level, that this fraction provides access of cholesterol to a blood vessels and organs. Determination of LDL is very informative for child organism. The deviations from the reference of this signs can indicate the risk of atherosclerosis and coronary heart disease in adulthood with high degree of probability.
The data of IA in 2.97 times higher in patients with PAH to the control group (2.67 and 0.90) according to our data. Average values of uric acid (UA) in the blood (0.26 ± 0.02 mmol/l and 0.19 ± 0.01 mmol/l, respectively, p < 0.001) and urine (3.28 ± 0.08 mmol/day and 2.24 ± 0.02 mmol/day, respectively, p < 0.001) in children with PAH were significantly higher than those of children in the control group. Hyperuricemia (> 0.32 mmol/l) was found in 2 girls — 4.80 % in boys, elevated levels of UA were found only in the one case — 2.50 %. We can say that the level of values fractions of cholesterol are the risk of PAH, analyzed of lipid metabolism, which are an indication for the possibility of correction. All these next biochemical tests in children with group observation were within the age norm.
Study of hemostasiogram is an important test of the origin and development of PAH and is potentially atherosclerosis and coronary heart disease to. We received the following data as result of research. Changes in hemostasiogram were indicated in 54.00 % of children. Major violations were characterized by reliable estimates an increase of activated recalcification time in the group of children with PAH in comparison with the control group (74.76 ± 5.06 sec to 64.76 ± 2.04 sec, p < 0.05) with increasing concentration of fibrinogen (17.53 ± 1.63 to 11.32 ± 0.77, p < 0.001) too, which may presented a predisposition to thrombogenesis in children with PAH group. The growth of the concentration of fibrinogen in plasma correlate with an increased risk of complications of heart disease within the reference values, according to the literature data even.
In the examined contingent we conducted a survey to for identify disorders of mineral metabolism child’s organism. This mineral metabolism data are presented in Table 4.
/41/41.jpg)
The levels of all minerals were identified within reference values. Significant difference observed in the level of sodium in children with PAH and the control group (respectively 133.90 ± 1.72 mmol/l and 119.16 ± 2.01 mmol/l, p < 0.001). But all numerical values varied within a reference.
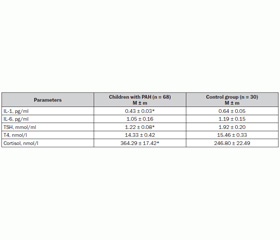
Investigation of hormonal levels, cytokine profile (IL-1, IL-6) in children with PAH presented in the Table 5.
Endothelial cells are active producers of IL-1. Complect of different types of cells which have receptors to IL-1 are numerous and distributed on the all organism systems. Growth stimulatory effect of IL-1 on the B cells is important for the development of the immune answer. Some effects caused by IL-6 are similar to the action of IL-1. The main effect of IL-6 is related to his participation as a cofactor in the differentiation of B lymphocytes and their maturation and transformation into plasmatic cells, which do immunoglobulin secretion. IL-6 is one of the most active cytokines which participated in the realization of immune answer. These cytokines contribute to the development of endothelial inflammation by activating endothelial cells, macrophages, stimulating production of free radicals, proteolytic enzymes and a significant increase coagulation activity. The levels of IL-1 and IL-6 were in the range of reference values with tendency to the lower level, especially IL-1, according to our data This fact indicates decrease of production of interleukins in child’s organism of the patients with PAH what confirmed by the above described clinical and laboratory effects. There are a significant decrease in TSH and absolute decrease in the level of T4. Their influence on lipid metabolism caused by inhibition of synthesis and increased fat splitting with the release of glycerol and fatty acids and increase the concentration of cholesterol. These data are consistent with our result (4.44 ± 0.10 mmol/l to 3.21 ± 0.26 mmol/l; p < 0.001). Cortisol has nonpresentive mineralocorticoid influence, but high maintenance caused by excessive sodium retention in the child organism (133.90 ± 1.72 mmol/l to the control group — 119.16 ± 2.01 mmol/l; p < 0.001). There is a clear tendency of significant relationships although but our data vary within the reference values.
Correlation analysis of our study data demonstrated a direct relationship between the value of IL-6 which correlated with the level of glucose (r = 0.65). SAT has a high degree of feedback to the level of T4. The value of IL-6 correlated in inverse proportion to the level of TSH (r = –0.31). TSH is also directly dependent from the levels of total protein (r = 0.79), which has negative relationship with sodium (r = –0.89). The level of calcium has negative relationship with the level of sodium (r = –0.85).
Conclusions
In patients with hypertension which PAH debuted in adolescence and have changes in lipid profile are formed pathological process in two ways: first way presented increase in total cholesterol associated with lower HDL fraction of cholesterol, and other — is an increase of Triglycerides with decreased level of HDL cholesterol, according to data of M.M. Korenev et al. (2010, 2011). These changes in lipid profile is prognostically unfavorable signs of atherosclerosis which formed in the patients (1st way), in others — is development of the metabolic syndrome in the young age (14–15 years), which we observed in our research. In children with PAH increase Triglyceride levels (1.96 ± 0.04 mmol/l) associated with significant decrease in HDL cholesterol fraction (1.20 ± 0.31 mmol/l) which predicts of development of the metabolic syndrome in the young age.
1. Коваленко В.М., Корнацький В.М., Дорогой А.П. та ін. Стан серцево-судинної патології та шляхи його покращення в Україні: Методичний посібник. — К., 2003. — 45 с.
2. Маколкин В.И. Метаболический синдром / В.И. Маколкин. — М.: МИА, 2010. — 142 c.
3. Collins R.T. Pre-hypertension and hypertension in pediatrics: don’t let the statistics hide the pathology / R.T. Collins, B.S. Alpert // J. Pediatr. — 2009. — Vol. 155, № 2. — P. 165-169.